

Health Coaching and Chronic Obstructive Pulmonary Disease Rehospitalization. A Randomized Study
- PMID: 26953637
- PMCID: PMC5027231
- DOI: 10.1164/rccm.201512-2503OC
Health Coaching and Chronic Obstructive Pulmonary Disease Rehospitalization. A Randomized Study
Abstract
Rationale: Hospital readmission for chronic obstructive pulmonary disease (COPD) has attracted attention owing to the burden to patients and the health care system. There is a knowledge gap on approaches to reducing COPD readmissions.
Objectives: To determine the effect of comprehensive health coaching on the rate of COPD readmissions.
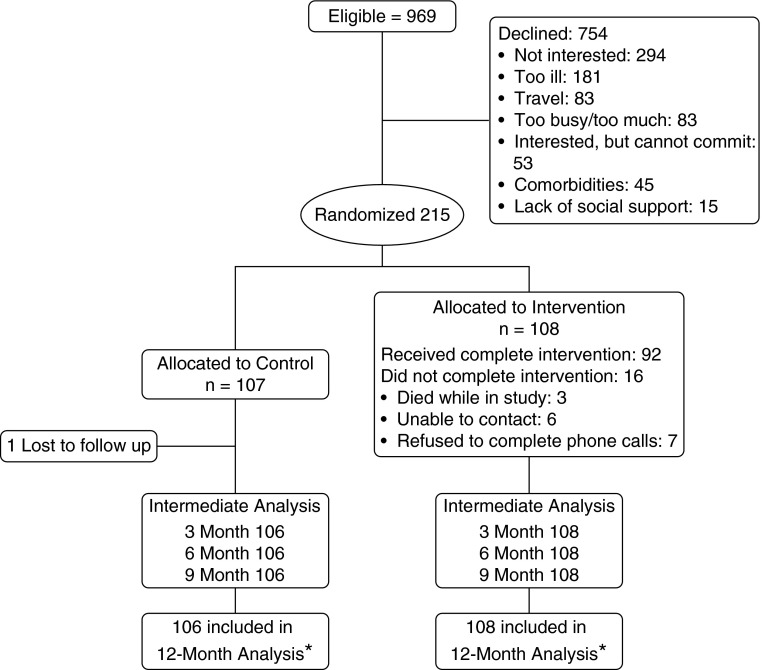
Methods: A total of 215 patients hospitalized for a COPD exacerbation were randomized at hospital discharge to receive either (1) motivational interviewing-based health coaching plus a written action plan for exacerbations (the use of antibiotics and oral steroids) and brief exercise advice or (2) usual care.
Measurements and main results: We evaluated the rate of COPD-related hospitalizations during 1 year of follow-up. The absolute risk reductions of COPD-related rehospitalization in the health coaching group were 7.5% (P = 0.01), 11.0% (P = 0.02), 11.6% (P = 0.03), 11.4% (P = 0.05), and 5.4% (P = 0.24) at 1, 3, 6, 9, and 12 months, respectively, compared with the control group. The odds ratios for COPD hospitalization in the intervention arm compared with the control arm were 0.09 (95% confidence interval [CI], 0.01-0.77) at 1 month postdischarge, 0.37 (95% CI, 0.15-0.91) at 3 months postdischarge, 0.43 (95% CI, 0.20-0.94) at 6 months postdischarge, and 0.60 (95% CI, 0.30-1.20) at 1 year postdischarge. The missing value rate for the primary outcome was 0.4% (one patient). Disease-specific quality of life improved significantly in the health coaching group compared with the control group at 6 and 12 months, based on the Chronic Respiratory Disease Questionnaire emotional score (emotion and mastery domains) and physical score (dyspnea and fatigue domains) (P < 0.05). There were no differences between groups in measured physical activity at any time point.
Conclusions: Health coaching may represent a feasible and possibly effective intervention designed to reduce COPD readmissions. Clinical trial registered with www.clinicaltrials.gov (NCT01058486).
Keywords: chronic obstructive pulmonary disease; communication skills; health coaching; hospitalizations; quality of life.
Figures
Comment in
-
Health Coaching: Another Component of Personalized Medicine for Patients with Chronic Obstructive Pulmonary Disease.Am J Respir Crit Care Med. 2016 Sep 15;194(6):647-9. doi: 10.1164/rccm.201604-0696ED. Am J Respir Crit Care Med. 2016. PMID: 27628071 No abstract available.
References
-
- Almagro P, Barreiro B, Ochoa de Echaguen A, Quintana S, Rodríguez Carballeira M, Heredia JL, Garau J. Risk factors for hospital readmission in patients with chronic obstructive pulmonary disease. Respiration. 2006;73:311–317. - PubMed
-
- Medicare Payment Advisory Commission (Medpac)Report to the Congress: promoting greater efficiency in Medicare. Washington, DC: Medpac; June 2007 [accessed 2016 Mar 16]. Available from: http://www.medpac.gov/documents/reports/Jun07_EntireReport.pdf
-
- Elixhauser A, Au DH, Podulka J.Readmissions for chronic obstructive pulmonary disease, 2008. Statistical Brief 121. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville, MD: Agency for Health Care Policy and Research; September 2011 [accessed 2016 Mar 16]. Available from: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb121.pdf
-
- Kasper EK, Gerstenblith G, Hefter G, Van Anden E, Brinker JA, Thiemann DR, Terrin M, Forman S, Gottlieb SH. A randomized trial of the efficacy of multidisciplinary care in heart failure outpatients at high risk of hospital readmission. J Am Coll Cardiol. 2002;39:471–480. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
