

Erythrocyte sedimentation rate and C-reactive protein to monitor treatment outcomes in diabetic foot osteomyelitis
- PMID: 26953894
- PMCID: PMC7950144
- DOI: 10.1111/iwj.12574
Erythrocyte sedimentation rate and C-reactive protein to monitor treatment outcomes in diabetic foot osteomyelitis
Abstract
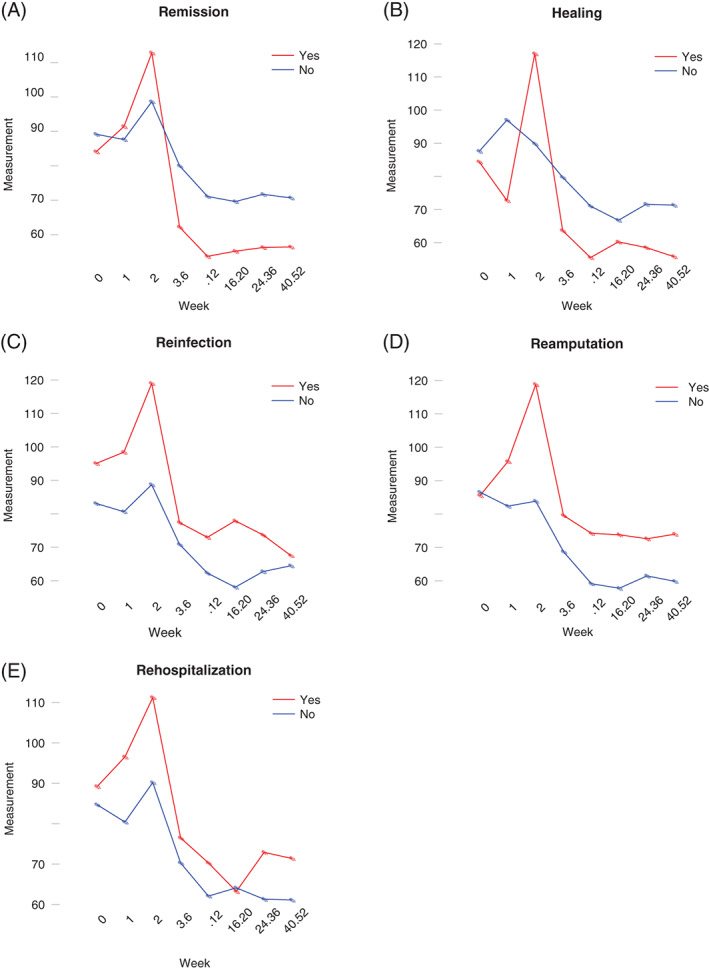
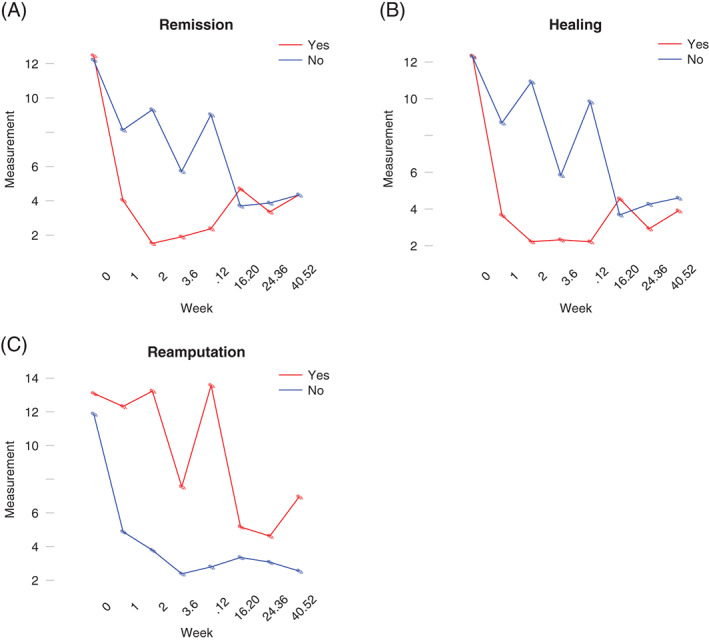
This study sought to evaluate the effectiveness of the inflammatory markers, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), in monitoring treatment of osteomyelitis in the diabetic foot. We screened 150 charts of patients admitted to our hospital with diabetic foot osteomyelitis (DFO), confirmed by positive results of bone culture and/or histopathology. We included patients who had an initial ESR/CRP within 72 hours of admission and two reported follow-up values. We dichotomised patients based on the outcomes wound healing, re-infection, recurrent ulceration, re-hospitalisation, additional surgery, re-amputation and death, all within 12 months, and analysed the trajectories of the markers over time. Our primary outcome, DFO remission, was defined as wound healing within 12 months of follow-up without re-infection. We included 122 subjects; 65 patients (53·3%) had a combination of positive culture and histopathology. Factors associated with DFO remission (n = 46) were a lower white blood count (WBC) at admission (P = 0·006) and a higher glomerular filtration rate (GFR, P = 0·049). Factors associated with healing were a lower WBC (P = 0·004), a higher GFR (P = 0·01), longer wound duration before admission (P = 0·01), location of the ulcer on the great toe (P = 0·01) and higher glycated haemoglobin (P = 0·03). Logistic regression analysis demonstrated no associations between DFO remission and other variables collected. Trajectories of the inflammatory markers showed an association between stagnating values of ESR and CRP and poor clinical outcomes. In this study population, the trajectories of both ESR and CRP during 12 months follow-up suggest a predictive role of both inflammatory markers when monitoring treatment of DFO.
Keywords: Biomarkers; C-reactive protein; Diabetic foot infection; Erythrocyte sedimentation rate; Osteomyelitis.
© 2016 Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Figures
References
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, Lin JK, Farzadfar F, Khang YH, Stevens GA, Rao M, Ali MK, Riley LM, Robinson CA, Ezzati M. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country‐years and 2·7 million participants. Lancet 2011;378:31–40. - PubMed
-
- Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010;87:4–14. - PubMed
-
- Lavery LA, Peters EJG, Armstrong DG, Wendel CS, Murdoch DP, Lipsky BA. Risk factors for developing osteomyelitis in patients with diabetic foot wounds. Diabetes Res Clin Pract 2009;83:347–52. - PubMed
-
- Berendt AR, Peters EJ, Bakker K, Embil JM, Eneroth M, Hinchliffe RJ, Jeffcoate WJ, Lipsky BA, Senneville E, Teh J, Valk GD. Diabetic foot osteomyelitis: a progress report on diagnosis and a systematic review of treatment. Diabetes Metab Res Rev 2008;24:S145–61. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
