

Cardiovascular and Renal Outcomes of Renin-Angiotensin System Blockade in Adult Patients with Diabetes Mellitus: A Systematic Review with Network Meta-Analyses
- PMID: 26954482
- PMCID: PMC4783064
- DOI: 10.1371/journal.pmed.1001971
Cardiovascular and Renal Outcomes of Renin-Angiotensin System Blockade in Adult Patients with Diabetes Mellitus: A Systematic Review with Network Meta-Analyses
Erratum in
-
Correction: Cardiovascular and Renal Outcomes of Renin-Angiotensin System Blockade in Adult Patients with Diabetes Mellitus: A Systematic Review with Network Meta-Analyses.PLoS Med. 2016 Jun 10;13(6):e1002064. doi: 10.1371/journal.pmed.1002064. eCollection 2016 Jun. PLoS Med. 2016. PMID: 27284684 Free PMC article.
Abstract
Background: Medications aimed at inhibiting the renin-angiotensin system (RAS) have been used extensively for preventing cardiovascular and renal complications in patients with diabetes, but data that compare their clinical effectiveness are limited. We aimed to compare the effects of classes of RAS blockers on cardiovascular and renal outcomes in adults with diabetes.
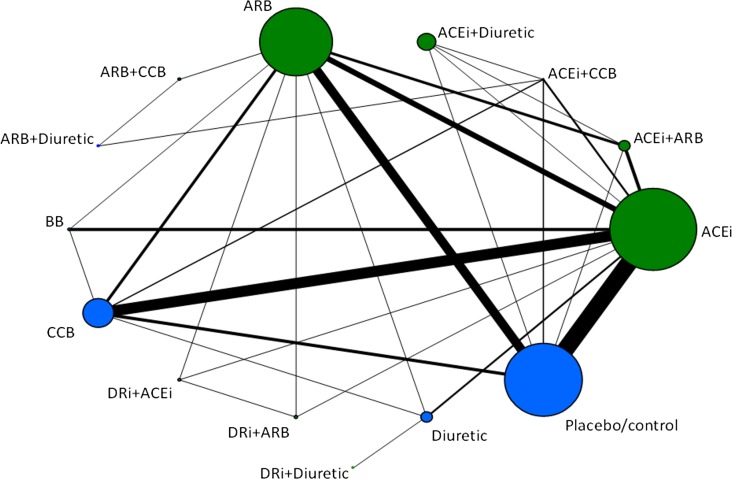
Methods and findings: Eligible trials were identified by electronic searches in PubMed/MEDLINE and the Cochrane Database of Systematic Reviews (1 January 2004 to 17 July 2014). Interventions of interest were angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), and direct renin (DR) inhibitors. The primary endpoints were cardiovascular mortality, myocardial infarction, and stroke-singly and as a composite endpoint, major cardiovascular outcome-and end-stage renal disease [ESRD], doubling of serum creatinine, and all-cause mortality-singly and as a composite endpoint, progression of renal disease. Secondary endpoints were angina pectoris and hospitalization for heart failure. In all, 71 trials (103,120 participants), with a total of 14 different regimens, were pooled using network meta-analyses. When compared with ACE inhibitor, no other RAS blocker used in monotherapy and/or combination was associated with a significant reduction in major cardiovascular outcomes: ARB (odds ratio [OR] 1.02; 95% credible interval [CrI] 0.90-1.18), ACE inhibitor plus ARB (0.97; 95% CrI 0.79-1.19), DR inhibitor plus ACE inhibitor (1.32; 95% CrI 0.96-1.81), and DR inhibitor plus ARB (1.00; 95% CrI 0.73-1.38). For the risk of progression of renal disease, no significant differences were detected between ACE inhibitor and each of the remaining therapies: ARB (OR 1.10; 95% CrI 0.90-1.40), ACE inhibitor plus ARB (0.97; 95% CrI 0.72-1.29), DR inhibitor plus ACE inhibitor (0.99; 95% CrI 0.65-1.57), and DR inhibitor plus ARB (1.18; 95% CrI 0.78-1.84). No significant differences were showed between ACE inhibitors and ARBs with respect to all-cause mortality, cardiovascular mortality, myocardial infarction, stroke, angina pectoris, hospitalization for heart failure, ESRD, or doubling serum creatinine. Findings were limited by the clinical and methodological heterogeneity of the included studies. Potential inconsistency was identified in network meta-analyses of stroke and angina pectoris, limiting the conclusiveness of findings for these single endpoints.
Conclusions: In adults with diabetes, comparisons of different RAS blockers showed similar effects of ACE inhibitors and ARBs on major cardiovascular and renal outcomes. Compared with monotherapies, the combination of an ACE inhibitor and an ARB failed to provide significant benefits on major outcomes. Clinicians should discuss the balance between benefits, costs, and potential harms with individual diabetes patients before starting treatment.
Review registration: PROSPERO CRD42014014404.
Conflict of interest statement
BH has previously received funds for methodologic advice from Amgen Canada and Cornerstone Research Group for the provision of advice related to systematic reviews and meta-analysis. None of the advice is related to the content of this manuscript. All the other authors have declared that no competing interests exist.
Figures
Similar articles
-
Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers for adults with early (stage 1 to 3) non-diabetic chronic kidney disease.Cochrane Database Syst Rev. 2011 Oct 5;(10):CD007751. doi: 10.1002/14651858.CD007751.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2023 Jul 19;7:CD007751. doi: 10.1002/14651858.CD007751.pub3. PMID: 21975774 Updated.
-
Renin-Angiotensin System Inhibitors and Kidney and Cardiovascular Outcomes in Patients With CKD: A Bayesian Network Meta-analysis of Randomized Clinical Trials.Am J Kidney Dis. 2016 May;67(5):728-41. doi: 10.1053/j.ajkd.2015.10.011. Epub 2015 Nov 18. Am J Kidney Dis. 2016. PMID: 26597926
-
ACE Inhibitor Benefit to Kidney and Cardiovascular Outcomes for Patients with Non-Dialysis Chronic Kidney Disease Stages 3-5: A Network Meta-Analysis of Randomised Clinical Trials.Drugs. 2020 Jun;80(8):797-811. doi: 10.1007/s40265-020-01290-3. Drugs. 2020. PMID: 32333236 Free PMC article.
-
Effects of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers on All-Cause Mortality and Renal Outcomes in Patients with Diabetes and Albuminuria: a Systematic Review and Meta-Analysis.Kidney Blood Press Res. 2018;43(3):768-779. doi: 10.1159/000489913. Epub 2018 May 22. Kidney Blood Press Res. 2018. PMID: 29794446
-
Beta-blockers and inhibitors of the renin-angiotensin aldosterone system for chronic heart failure with preserved ejection fraction.Cochrane Database Syst Rev. 2018 Jun 28;6(6):CD012721. doi: 10.1002/14651858.CD012721.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 May 22;5:CD012721. doi: 10.1002/14651858.CD012721.pub3. PMID: 29952095 Free PMC article. Updated.
Cited by
-
Impacts of renin-angiotensin system inhibitors on two-year clinical outcomes in diabetic and dyslipidemic acute myocardial infarction patients after a successful percutaneous coronary intervention using newer-generation drug-eluting stents.Medicine (Baltimore). 2020 Jul 24;99(30):e21289. doi: 10.1097/MD.0000000000021289. Medicine (Baltimore). 2020. PMID: 32791710 Free PMC article.
-
Renin-Angiotensin-Aldosterone System Modulators in Adults with Hypertension: A Network Meta-Analysis of Randomized Controlled Trials.Drugs. 2024 Nov;84(11):1445-1462. doi: 10.1007/s40265-024-02092-7. Epub 2024 Sep 23. Drugs. 2024. PMID: 39312177
-
Sodium-glucose cotransporter 2 inhibitors and contrast-induced nephropathy risk: a meta-analysis.Eur J Clin Pharmacol. 2025 Mar;81(3):337-345. doi: 10.1007/s00228-024-03799-y. Epub 2024 Dec 27. Eur J Clin Pharmacol. 2025. PMID: 39729107
-
10. Cardiovascular Disease and Risk Management: Standards of Care in Diabetes-2023.Diabetes Care. 2023 Jan 1;46(Suppl 1):S158-S190. doi: 10.2337/dc23-S010. Diabetes Care. 2023. PMID: 36507632 Free PMC article. Review.
-
Development and Validation of a Medication Selection Model Under Clinical Application of Renin-Angiotensin Inhibitor Combined with Calcium Channel Blocker for Hypertension Patients.Med Sci Monit. 2020 Apr 14;26:e923696. doi: 10.12659/MSM.923696. Med Sci Monit. 2020. PMID: 32285846 Free PMC article.
References
-
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries for 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. 10.1016/S0140-6736(15)60692-4 - DOI - PMC - PubMed
-
- GBD 2013 DALYs and HALE Collaborators, Murray CJ, Barber RM, Foreman KJ, Abbasoglu Ozgoren A, Abd-Allah F, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet. 2015;386:2145–2191. 10.1016/S0140-6736(15)61340-X - DOI - PMC - PubMed
-
- Sanders GD, Coeytaux R, Dolor RJ, Hasselblad V, Patel UD, Powers B, et al. Angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor antagonists (ARBs), and direct renin inhibitors for treating essential hypertension: an update 2011. June [cited 25 Jul 2015]. Rockville (Maryland): Agency for Healthcare Research and Quality. Available: http://www.ncbi.nlm.nih.gov/books/NBK61789/. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
