

Host Immune Response to Clostridium difficile Infection in Inflammatory Bowel Disease Patients
- PMID: 26954708
- PMCID: PMC4792680
- DOI: 10.1097/MIB.0000000000000696
Host Immune Response to Clostridium difficile Infection in Inflammatory Bowel Disease Patients
Abstract
Background: Clostridium difficile infection (CDI) affects patients with inflammatory bowel disease (IBD). The aim of this study was to compare humoral response to C. difficile toxins in IBD patients and control outpatients.
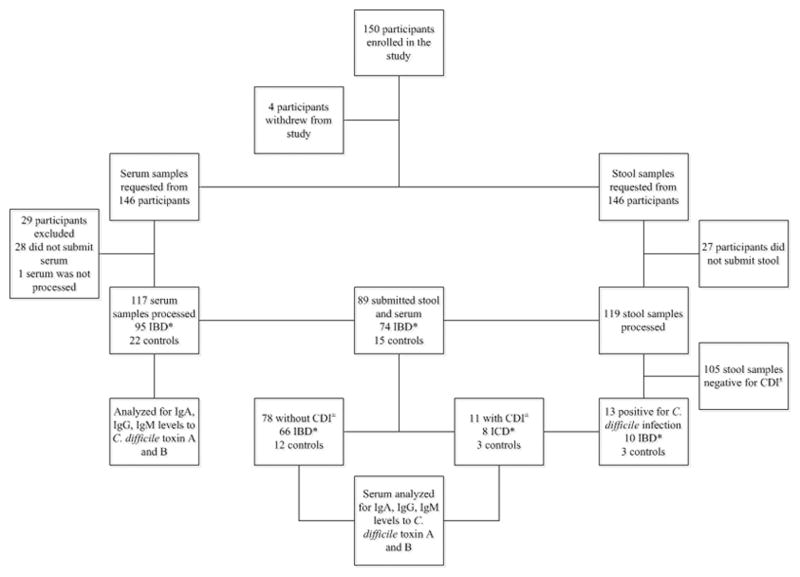
Methods: We prospectively followed adult IBD patients and control subjects with serum and stool samples obtained at enrollment and during periods of CDI and tested by PCR. Semiquantitative serum levels of IgM, IgG, and IgA to C. difficile toxins A and B were measured.
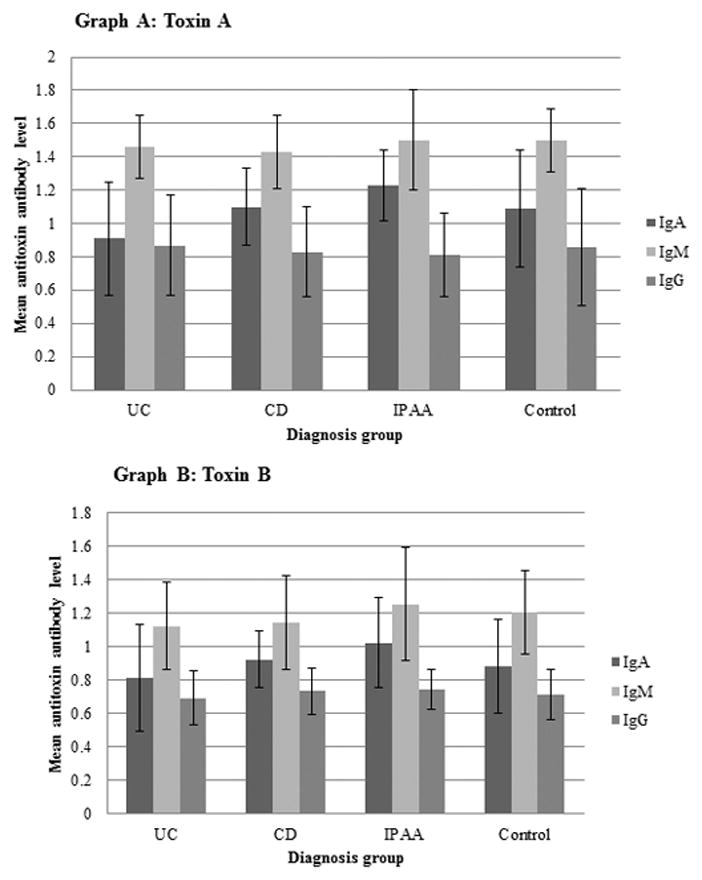
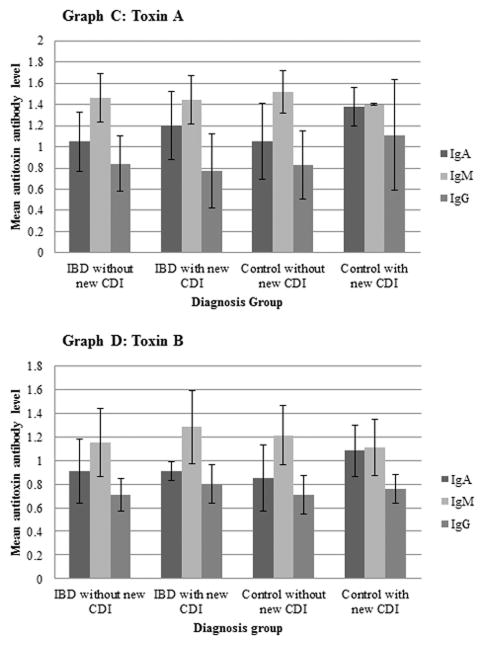
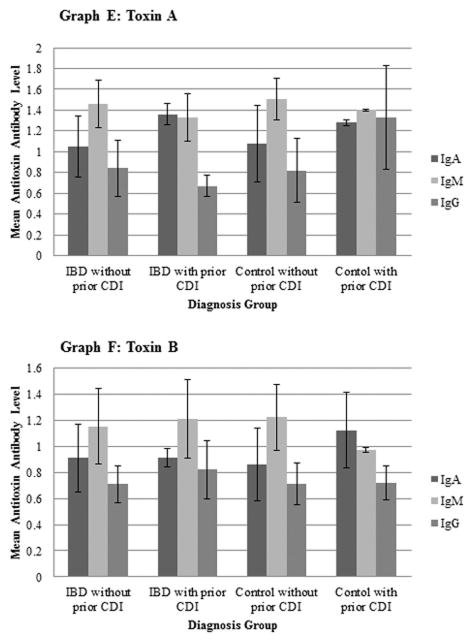
Results: Overall, 119 stool and 117 serum samples were obtained from 150 subjects. Different levels of IgA to toxin A (P = 0.0016) and toxin B (P = 0.0468) were noted between different IBD groups. Toxin A IgA levels were higher in the Crohn's disease group (P = 0.0321) and ileal pouch anal anastomosis (IPAA) group (P = 0.001) compared with the ulcerative colitis (UC) group, and toxin B IgA levels were higher in the IPAA group compared with the UC group (P = 0.0309). There were lower levels of toxin A IgA in IBD patients compared with those in subjects without new CDI (P = 0.0488) and higher levels in IBD patients with compared with those in subjects without CDI history before enrollment (P = 0.016). There were nonsignificant lower toxin A IgG levels in IBD patients compared with those in subjects without prior CDI (P = 0.095) and higher levels in control subjects with a history of CDI compared with IBD patients with prior CDI (P = 0.049).
Conclusions: Patients with UC have lower IgA levels to C. difficile toxins compared with those with Crohn's disease and those after IPAA. Patients with IBD with prior CDI failed to demonstrate any increase in antitoxin IgG. Our findings suggest that IBD patients may benefit from immunization strategies targeting C. difficile toxins.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention (CDC) Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep. 2012;61:157–162. - PubMed
-
- Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect. 1998;40:1–15. - PubMed
-
- Garey KW, Sethi S, Yadav Y, et al. Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J Hosp Infect. 2008;70:298–304. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
