

Intragastric Balloon for Overweight Patients
- PMID: 26955259
- PMCID: PMC4777670
- DOI: 10.4293/JSLS.2015.00107
Intragastric Balloon for Overweight Patients
Abstract
Background and objectives: Current treatments for overweight adults include reduced-calorie diet, exercise, behavior modification, and selective use of medications. Many achieve suboptimal results with these measures and progress to obesity. Whether the intragastric balloon (IGB), a reversible device approved for treatment of obesity, is a safe and effective option in overweight adults is less well studied. We conducted a study to prospectively analyze the safety and effectiveness of IGB in overweight adults, to compare the results to a simultaneously studied cohort of obese patients, and to share procedural tips for safe IGB placement and removal.
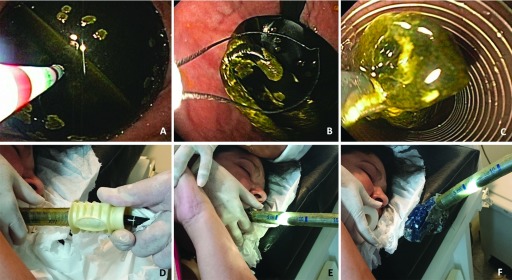
Methods: One hundred thirty-nine patients were evaluated in this prospective, nonrandomized study. Twenty-six overweight [body mass index (BMI), 26-30)] and 113 obese (BMI > 30) patients underwent outpatient, endoscopic IGB placement under intravenous sedation. The IGB was filled with a 550-900 mL (average, 640 mL) solution of saline, radiological contrast, and methylene blue, with an approximate final proportion of 65:2:1. The patients were followed up at 1-2 weeks and then monthly for 6 months. At 6 months, they underwent IGB removal via an esophageal overtube to optimize safety, and then they were observed for 6 more months.
Results: IGB time was 190 ± 36 d in the overweight patients and 192 ± 43 d in the obese patients. Symptoms of IGB intolerance included nausea and pain, which were transiently present in 50-95% of patients for several days, and necessitated early IGB removal in 6% of patients. There were no procedure-related complications and no IGB-related esophagitis, erosion, perforation, or obstruction. The percentage of excess weight loss (EWL%) was 96 ± 54% in the overweight group and 41 ± 26% in the obese group (P < 0.001).
Conclusion: In overweight adults failing standard treatments, IGB placement for 6 months had an acceptable safety profile and excellent weight loss.
Keywords: Endoscopic device; Intragastric balloon; Obesity; Overtube; Overweight.
Figures


Similar articles
-
Fluid-filled intragastric balloons are an effective and safe weight loss option across BMI and age ranges.Surg Endosc. 2022 Jul;36(7):5160-5166. doi: 10.1007/s00464-021-08892-2. Epub 2021 Nov 29. Surg Endosc. 2022. PMID: 34845556
-
Intragastric Balloon: a Retrospective Evaluation of 5874 Patients on Tolerance, Complications, and Efficacy in Different Degrees of Overweight.Obes Surg. 2020 Dec;30(12):4892-4898. doi: 10.1007/s11695-020-04985-4. Epub 2020 Sep 21. Obes Surg. 2020. PMID: 32959329
-
Real-World Safety and Efficacy of Fluid-Filled Dual Intragastric Balloon for Weight Loss.Clin Gastroenterol Hepatol. 2018 Jul;16(7):1081-1088.e1. doi: 10.1016/j.cgh.2018.02.026. Epub 2018 Mar 2. Clin Gastroenterol Hepatol. 2018. PMID: 29481969
-
Intragastric Balloon Treatment for Obesity: Review of Recent Studies.Adv Ther. 2017 Aug;34(8):1859-1875. doi: 10.1007/s12325-017-0562-3. Epub 2017 Jul 13. Adv Ther. 2017. PMID: 28707286 Review.
-
Efficacy of Intragastric Balloons for Weight Loss in Overweight and Obese Adults: a Systematic Review and Meta-analysis of Randomized Controlled Trials.Obes Surg. 2020 Jul;30(7):2743-2753. doi: 10.1007/s11695-020-04558-5. Obes Surg. 2020. PMID: 32300945
Cited by
-
Comorbidity Remission Following Intragastric Dual Balloon Placement.Obes Surg. 2019 Jan;29(1):353-355. doi: 10.1007/s11695-018-3564-6. Obes Surg. 2019. PMID: 30382461
-
Intra-gastric balloons - The past, present and future.Ann Med Surg (Lond). 2021 Feb 2;63:102138. doi: 10.1016/j.amsu.2021.01.086. eCollection 2021 Mar. Ann Med Surg (Lond). 2021. PMID: 33664941 Free PMC article. Review.
-
Medical Devices in Obesity Treatment.Curr Diab Rep. 2019 Aug 30;19(10):90. doi: 10.1007/s11892-019-1217-3. Curr Diab Rep. 2019. PMID: 31471810 Free PMC article. Review.
-
INTRAGASTRIC BALLOON AND IMPACT ON WEIGHT LOSS: EXPERIENCE IN QUITO, EQUADOR.Arq Bras Cir Dig. 2023 May 26;36:e1731. doi: 10.1590/0102-672020230002e1731. eCollection 2023. Arq Bras Cir Dig. 2023. PMID: 37255102 Free PMC article.
-
Safety, tolerability and efficacy of a novel self-use biodegradable device for management of obesity.Obes Sci Pract. 2019 Jun 25;5(4):376-382. doi: 10.1002/osp4.343. eCollection 2019 Aug. Obes Sci Pract. 2019. PMID: 31452922 Free PMC article.
References
-
- WHO. Obesity: preventing and managing the global epidemic. Report of a WHO Consultation. Health Organ Tech Rep Ser. 2000;894:1–253. - PubMed
-
- Buchwald H. The evolution of metabolic/bariatric surgery. Obes Surg. 2014;24:1126–1135. - PubMed
-
- Hainer V, Toplak H, Mitrakou A. Treatment modalities of obesity: what fits whom? Diabetes Care. 2008;31(Suppl 2):S269–S277. - PubMed
-
- Wolf AM, Woodworth KA. Obesity prevention: recommended strategies and challenges. Am J Med. 2009;122:S19–S23. - PubMed
-
- Neligan PJ, Williams N. Nonsurgical and surgical treatment of obesity. Anesthesiol Clin North Am. 2005;23:501–523. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical