

Prognostic factors affecting the risk of thoracic progression in extensive-stage small cell lung cancer
- PMID: 26955807
- PMCID: PMC4782389
- DOI: 10.1186/s12885-016-2222-4
Prognostic factors affecting the risk of thoracic progression in extensive-stage small cell lung cancer
Abstract
Background: The efficacy of combined modality therapy is evaluated for patients with extensive-stage (ES) small cell lung cancer (SCLC). This study evaluated prognostic factors affecting the risk of thoracic progression in ES-SCLC patients likely to undergo thoracic radiotherapy combined chemotherapy.
Methods: A retrospective review of ES-SCLC patients who had received systemic chemotherapy at our hospital was performed. Tumor size, metastatic sites, and laboratory data at diagnosis were evaluated as potential prognostic factors. In ES-SCLC patients without pleural dissemination, the rate of thoracic progression after initial chemotherapy was assessed.
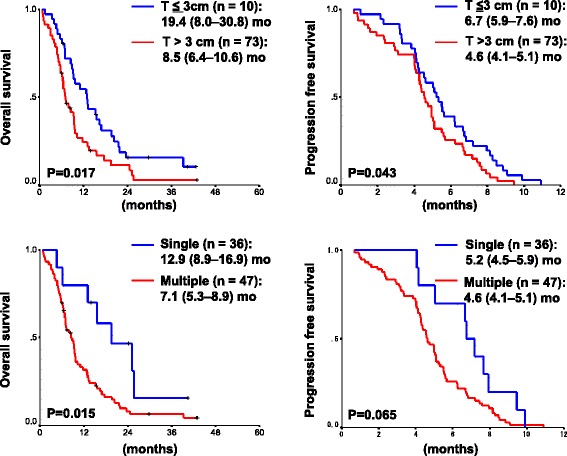
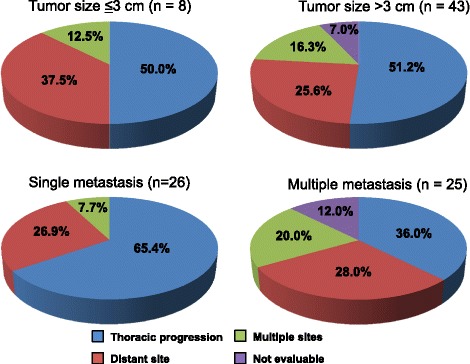
Results: Eighty-three of 96 consecutive ES-SCLC patients were analyzed. The overall response rate was 55 %, median progression free survival was 5.0 months (mo), and overall survival (OS) was 9.2 mo. Tumor size (19.4 mo for ≤3 cm vs. 8.5 mo for >3 cm, p = 0.017) and the number of metastatic sites (12.9 mo for single sites vs. 7.1 mo for multiple sites, p = 0.015) were prognostic factors, in addition to known prognostic factors such as performance status and the levels of LDH and sodium. Cox proportional hazard model showed that the OS was significantly worse in patients with large (>3 cm) primary tumor size {HR 2.44 [95 % confidential interval (CI) 1.05-5.68], p = 0.038} and multiple metastatic sites [HR 1.81 (95 % CI 1.08-3.04), p = 0.026]. In 51 cases without pleural dissemination, the number of metastatic sites was associated with thoracic progression after initial chemotherapy (65 % for single sites vs. 36 % for multiple sites, p = 0.036).
Conclusion: Large tumor size and multiple metastatic sites at diagnosis significantly predicted poor survival in ES-SCLC patients. Based on the high rate of thoracic progression in ES-SCLC patients with single site of distant metastasis, we should consider thoracic radiotherapy combined with chemotherapy for this population.
Figures
References
-
- Takada M, Fukuoka M, Kawahara M, Sugiura T, Yokoyama A, Yokota S, et al. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with cisplatin and etoposide for limited-stage small-cell lung cancer: results of the Japan Clinical Oncology Group Study 9104. J Clin Oncol Off J Am Soc Clin Oncol. 2002;20(14):3054–60. doi: 10.1200/JCO.2002.12.071. - DOI - PubMed
-
- De Ruysscher D, Pijls-Johannesma M, Bentzen SM, Minken A, Wanders R, Lutgens L, et al. Time between the first day of chemotherapy and the last day of chest radiation is the most important predictor of survival in limited-disease small-cell lung cancer. J Clin Oncol Off J Am Soc Clin Oncol. 2006;24(7):1057–63. doi: 10.1200/JCO.2005.02.9793. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
