

Cause of Death and Predictors of All-Cause Mortality in Anticoagulated Patients With Nonvalvular Atrial Fibrillation: Data From ROCKET AF
- PMID: 26955859
- PMCID: PMC4943233
- DOI: 10.1161/JAHA.115.002197
Cause of Death and Predictors of All-Cause Mortality in Anticoagulated Patients With Nonvalvular Atrial Fibrillation: Data From ROCKET AF
Abstract
Background: Atrial fibrillation is associated with higher mortality. Identification of causes of death and contemporary risk factors for all-cause mortality may guide interventions.
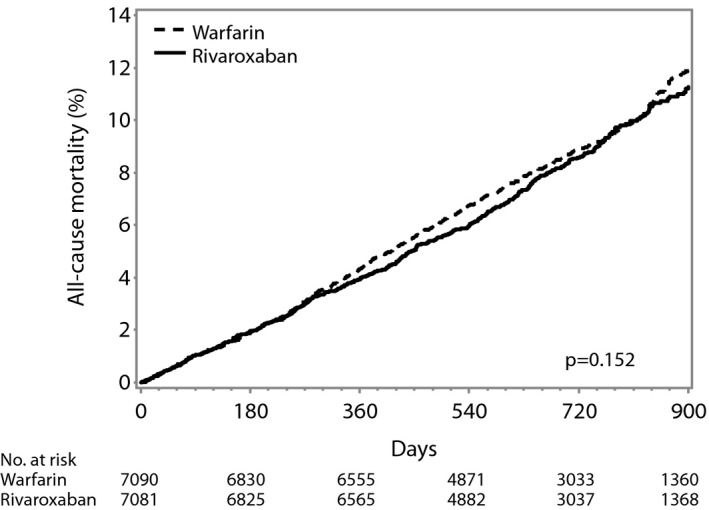
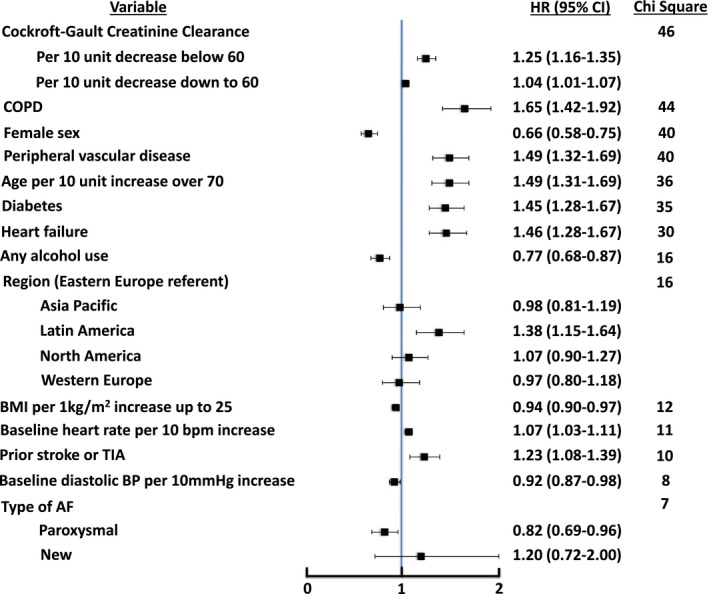
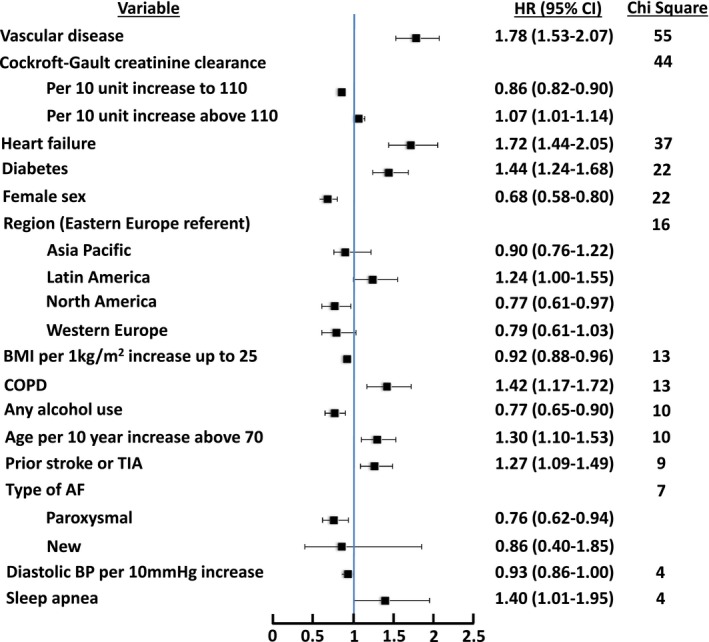
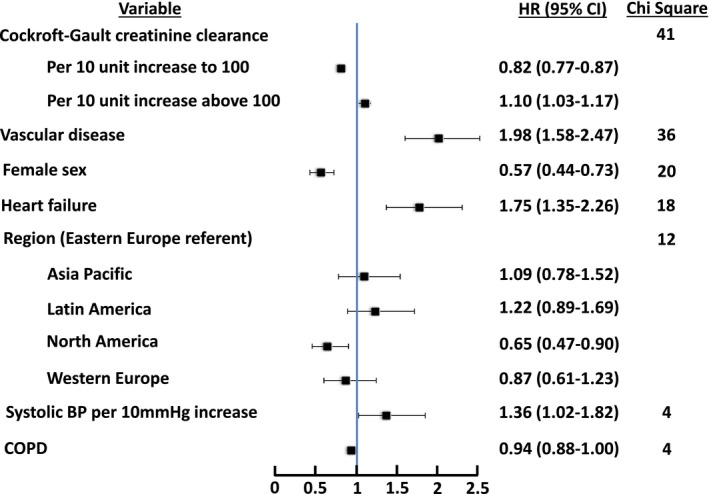
Methods and results: In the Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF) study, patients with nonvalvular atrial fibrillation were randomized to rivaroxaban or dose-adjusted warfarin. Cox proportional hazards regression with backward elimination identified factors at randomization that were independently associated with all-cause mortality in the 14 171 participants in the intention-to-treat population. The median age was 73 years, and the mean CHADS2 score was 3.5. Over 1.9 years of median follow-up, 1214 (8.6%) patients died. Kaplan-Meier mortality rates were 4.2% at 1 year and 8.9% at 2 years. The majority of classified deaths (1081) were cardiovascular (72%), whereas only 6% were nonhemorrhagic stroke or systemic embolism. No significant difference in all-cause mortality was observed between the rivaroxaban and warfarin arms (P=0.15). Heart failure (hazard ratio 1.51, 95% CI 1.33-1.70, P<0.0001) and age ≥75 years (hazard ratio 1.69, 95% CI 1.51-1.90, P<0.0001) were associated with higher all-cause mortality. Multiple additional characteristics were independently associated with higher mortality, with decreasing creatinine clearance, chronic obstructive pulmonary disease, male sex, peripheral vascular disease, and diabetes being among the most strongly associated (model C-index 0.677).
Conclusions: In a large population of patients anticoagulated for nonvalvular atrial fibrillation, ≈7 in 10 deaths were cardiovascular, whereas <1 in 10 deaths were caused by nonhemorrhagic stroke or systemic embolism. Optimal prevention and treatment of heart failure, renal impairment, chronic obstructive pulmonary disease, and diabetes may improve survival.
Clinical trial registration: URL: https://www.clinicaltrials.gov/. Unique identifier: NCT00403767.
Keywords: atrial fibrillation; mortality; rivaroxaban; stroke; warfarin.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population‐based study of the long‐term risks associated with atrial fibrillation: 20‐year follow‐up of the Renfrew/Paisley study. Am J Med. 2002;113:359–364. - PubMed
-
- Benjamin EJ, Wolf PA, D'Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–952. - PubMed
-
- Lloyd‐Jones DM, Larson MG, Leip EP, Beiser A, D'Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ, Levy D; Framingham Heart Study . Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002;106:3068–3072. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–988. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta‐analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
