

Somatic mosaicism due to a reversion variant causing hemi-atrophy: a novel variant of dystrophinopathy
- PMID: 26956251
- PMCID: PMC5027673
- DOI: 10.1038/ejhg.2016.22
Somatic mosaicism due to a reversion variant causing hemi-atrophy: a novel variant of dystrophinopathy
Abstract
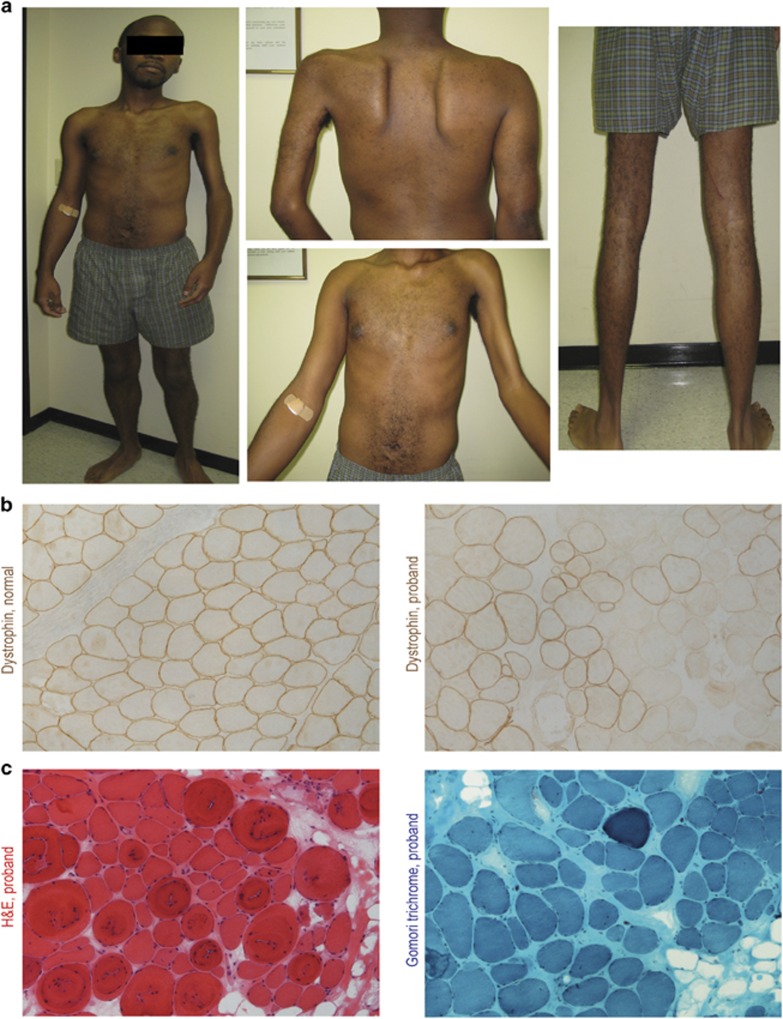
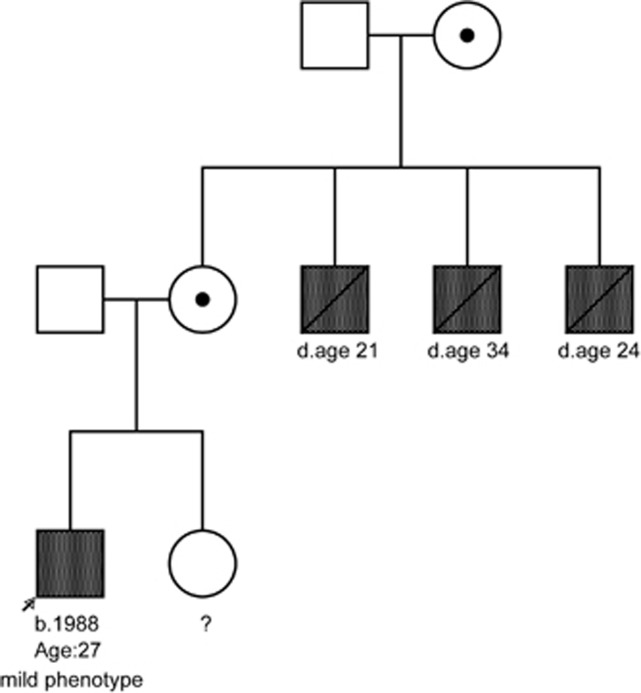
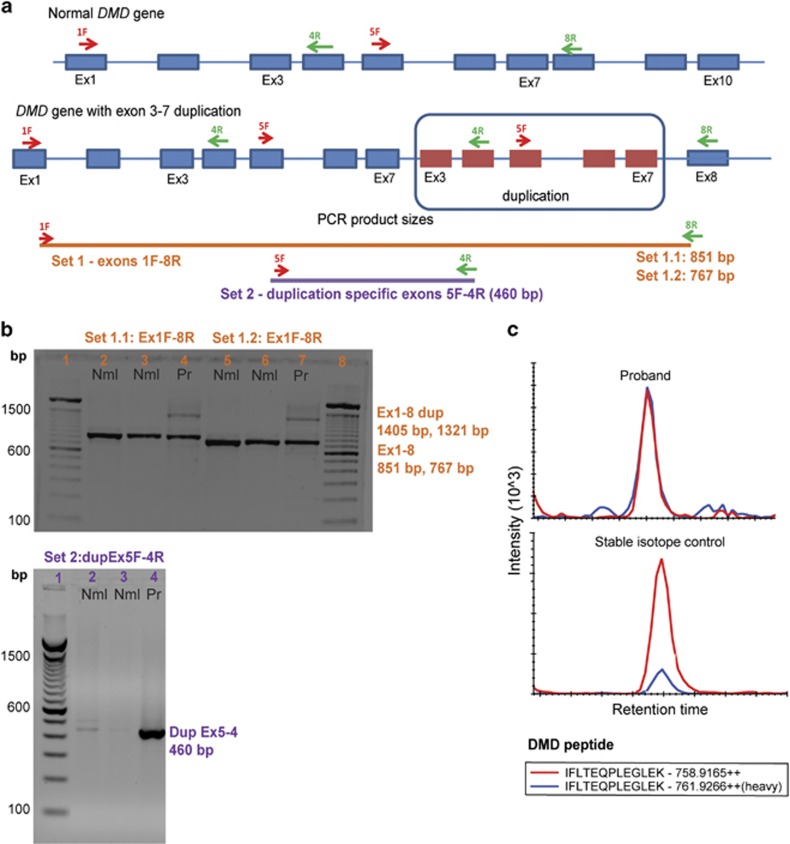
We describe a case of hemi-atrophy in a young adult male, with a positive family history of three maternal uncles with Duchenne muscular dystrophy (DMD). The patient showed progressive weakness localized to the left side, an abnormal electromyography, and creatine kinase levels >3000 IU/l. Muscle biopsy showed both dystrophin-positive and -negative myofibers. An out-of-frame duplication variant in DMD, that is, c.(93+1_94-1)_(649+1_650-1)dup(p.?) resulting in duplication of exons 3-7 was inherited, but the muscle biopsy showed dystrophin mRNA with and without the duplication. Dystrophin quantification using mass spectrometry showed 25% normal dystrophin protein levels in the muscle biopsy from the stronger right side. Sex chromosome aneuploidy was ruled out. We conclude that the patient inherited the duplication variant, but early in development an inner cell mass underwent a somatic recombination event removing the duplication and restoring dystrophin expression. To our knowledge, this is the first report of a reversion leading to somatic mosaicism in DMD.
Figures
References
-
- Hoffman EP, Brown RH, Kunkel LM: Dystrophin: the protein product of the Duchenne muscular dystrophy locus. Cell 1987; 51: 919–928. - PubMed
-
- Fanin M, Danieli GA, Vitiello L, Senter L, Angelini C: Prevalence of dystrophin-positive fibers in 85 Duchenne muscular dystrophy patients. Neuromuscul Disord 1992; 2: 41–45. - PubMed
-
- Hoffman EP, Morgan JE, Watkins SC, Partridge TA: Somatic reversion/suppression of the mouse mdx phenotype in vivo. J Neurol Sci 1990; 99: 9–25. - PubMed
-
- Yokota T, Lu QL, Morgan JE et al: Expansion of revertant fibers in dystrophic mdx muscles reflects activity of muscle precursor cells and serves as an index of muscle regeneration. J Cell Sci 2006; 119 (Pt 13): 2679–2687. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
