

Unusual renal tumour: multilocular cystic renal cell carcinoma
- PMID: 26957035
- PMCID: PMC4785450
- DOI: 10.1136/bcr-2016-214386
Unusual renal tumour: multilocular cystic renal cell carcinoma
Abstract
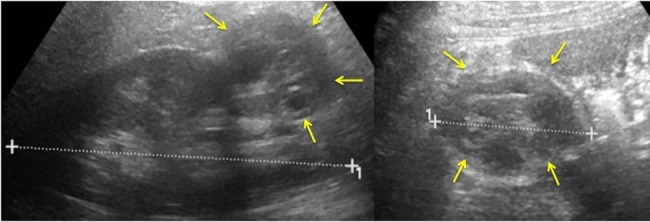
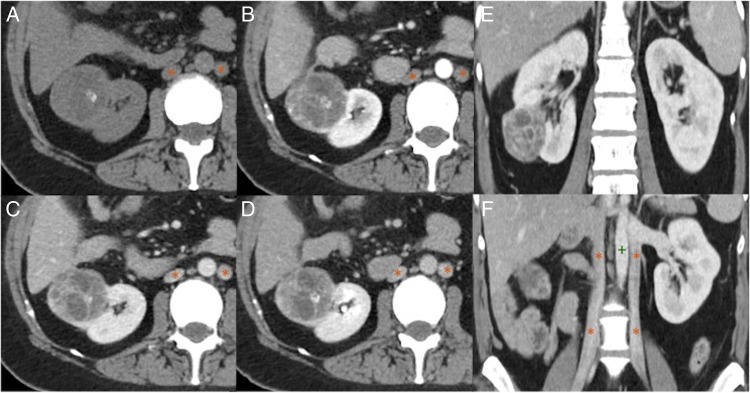
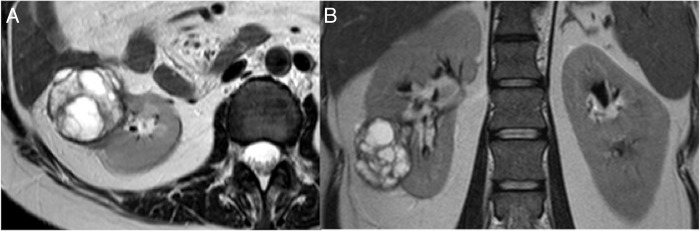
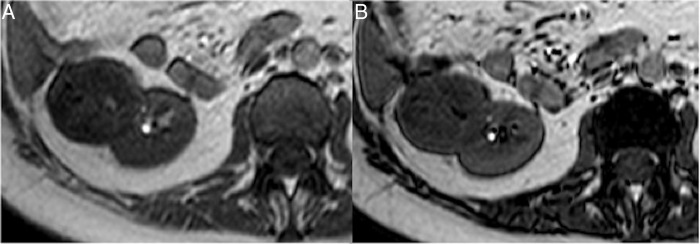
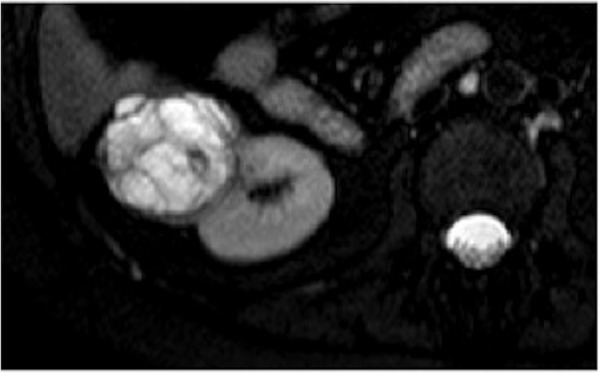
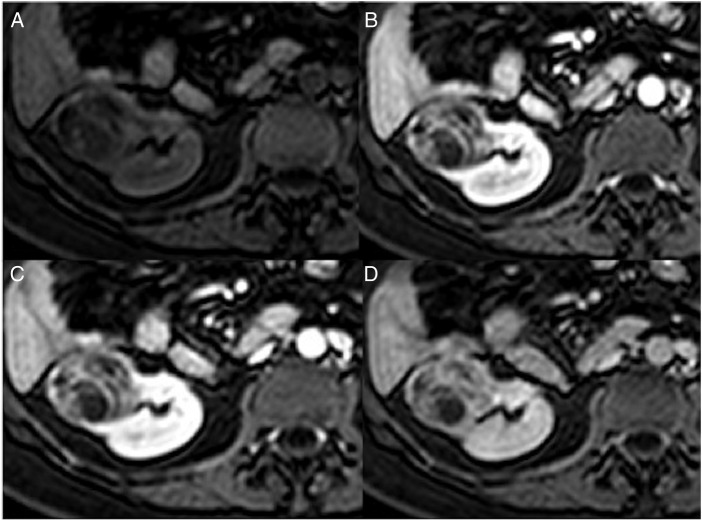
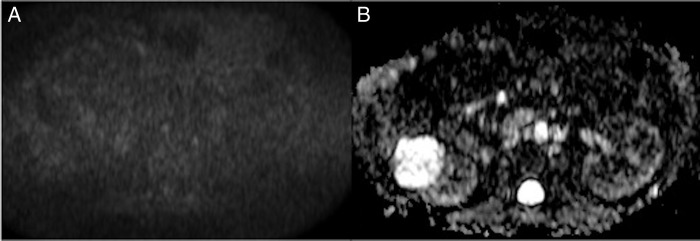
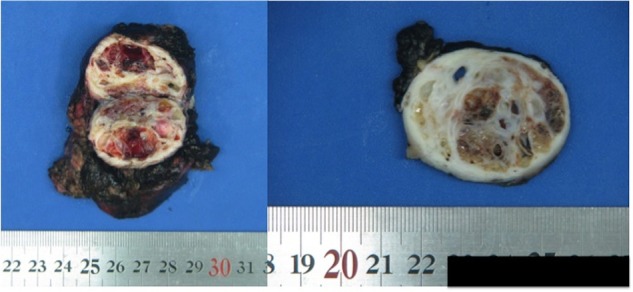
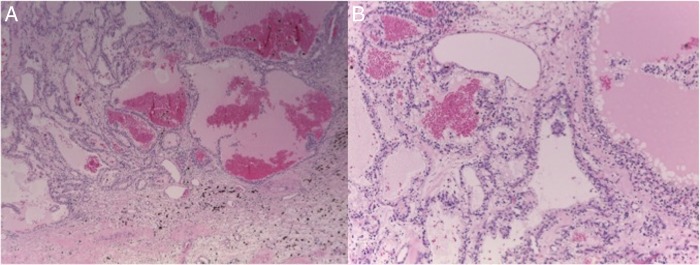
Multilocular cystic renal cell carcinoma (MCRCC) is a rare presentation of renal cell carcinoma. Most patients are asymptomatic and frequently MCRCCs are detected incidentally. MCRCCs have good prognosis because of their low malignant potential. We report a case of a 39-year-old woman who presented with mild right flank pain and normal laboratory data. On imaging examinations, a Bosniak III cystic lesion was detected in the lower third of the right kidney. She underwent right partial nephrectomy and histopathology showed a multilocular cystic renal cell carcinoma Fuhrman grade 1. In this article, we also present a review of the literature on MCRCC, highlight the correlation of the pathological and imaging characteristics of these low aggressive renal lesions, and underscore the importance of their recognition to prevent unnecessary radical surgery.
2016 BMJ Publishing Group Ltd.
Figures
Similar articles
-
[Clinical application of intraoperative ultrasonography for bilateral multilocular cystic renal cell carcinoma: a case report].Hinyokika Kiyo. 1998 Feb;44(2):97-100. Hinyokika Kiyo. 1998. PMID: 9546129 Review. Japanese.
-
Multilocular cystic renal cell carcinoma: a rare, unique entity and diagnostic challenge.Arch Iran Med. 2014 Feb;17(2):129-32. Arch Iran Med. 2014. PMID: 24527976
-
Cystic renal cell carcinomas in adults. Is preoperative recognition of multilocular cystic renal cell carcinoma possible?J Urol. 2005 Dec;174(6):2115-9. doi: 10.1097/01.ju.0000181210.72528.ab. J Urol. 2005. PMID: 16280739
-
Multilocular cystic renal cell carcinoma: clinicopathological features and preoperative prediction using multiphase computed tomography.BJU Int. 2011 Nov;108(9):1444-9. doi: 10.1111/j.1464-410X.2011.10247.x. Epub 2011 Jul 1. BJU Int. 2011. PMID: 21722289
-
Multilocular cystic renal cell carcinoma: a series of 12 cases and review of the literature.Urology. 2002 Sep;60(3):421-7. doi: 10.1016/s0090-4295(02)01742-9. Urology. 2002. PMID: 12350478 Review.
Cited by
-
Multilocular Cystic Renal Cell Carcinoma or Cystic Nephroma?Case Rep Urol. 2016;2016:5304324. doi: 10.1155/2016/5304324. Epub 2016 Dec 15. Case Rep Urol. 2016. PMID: 28074169 Free PMC article.
-
Multidetector CT Characteristics of Fumarate Hydratase-Deficient Renal Cell Carcinoma and Papillary Type II Renal Cell Carcinoma.Korean J Radiol. 2021 Dec;22(12):1996-2005. doi: 10.3348/kjr.2021.0212. Epub 2021 Sep 24. Korean J Radiol. 2021. PMID: 34668351 Free PMC article.
-
Solid renal masses in adults.Indian J Radiol Imaging. 2016 Oct-Dec;26(4):429-442. doi: 10.4103/0971-3026.195773. Indian J Radiol Imaging. 2016. PMID: 28104933 Free PMC article.
References
-
- Eble JN, Sauter G, Epstein JI et al. . Pathology and genetics of tumours of the urinary system and male genital organs. Lyon, France: IARC Press, 2004.
-
- Katabathina VS, Gangadhar K, Vinu-Nair S et al. . Cystic renal neoplasms in adults: current imaging update. Appl Radiol 2015;2015:23–33.
-
- Hora M, Hes O, Michal M et al. . Extensively cystic renal neoplasms in adults (Bosniak classification II or III)—possible “common” histological diagnoses: multilocular cystic renal cell carcinoma, cystic nephroma, and mixed epithelial and stromal tumor of the kidney. Int Urol Nephrol 2005;37:743–50. 10.1007/s11255-005-1201-5 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical