

Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Variceal Hemorrhage
- PMID: 26957908
- PMCID: PMC4781762
- DOI: 10.3348/kjr.2016.17.2.230
Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Variceal Hemorrhage
Abstract
Objective: To evaluate the feasibility, safety, and clinical outcomes of plug-assisted retrograde transvenous obliteration (PARTO) to treat gastric variceal hemorrhage in patients with portal hypertension.
Materials and methods: From May 2012 to June 2014, 19 patients (11 men and 8 women, median age; 61, with history of gastric variceal hemorrhage; 17, active bleeding; 2) who underwent PARTO using a vascular plug and a gelfoam pledget were retrospectively analyzed. Clinical and laboratory data were examined to evaluate primary (technical and clinical success, complications) and secondary (worsening of esophageal varix [EV], change in liver function) end points. Median follow-up duration was 11 months, from 6.5 to 18 months. The Wilcoxon signed-rank test was used to compare laboratory data before and after the procedure.
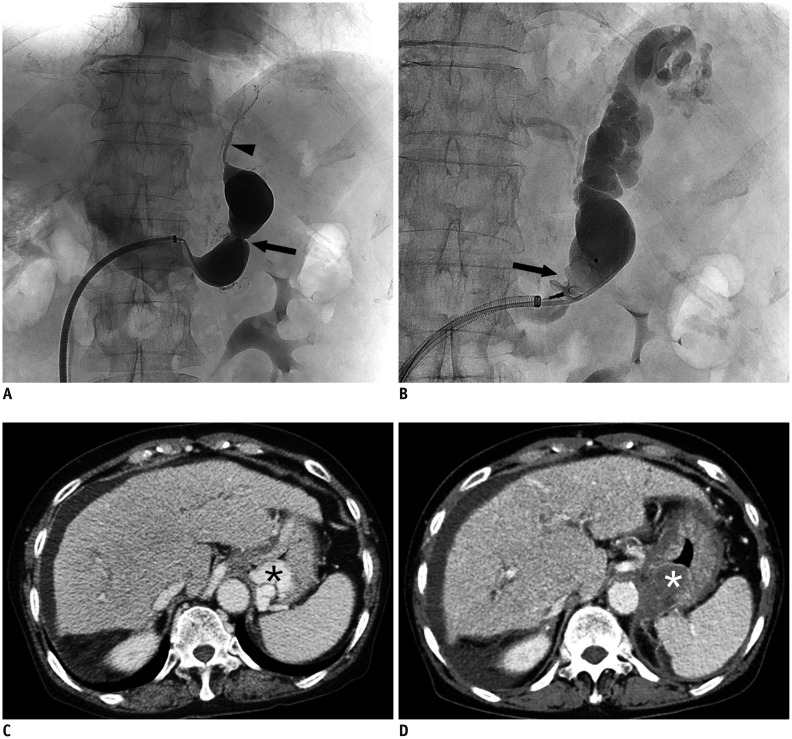
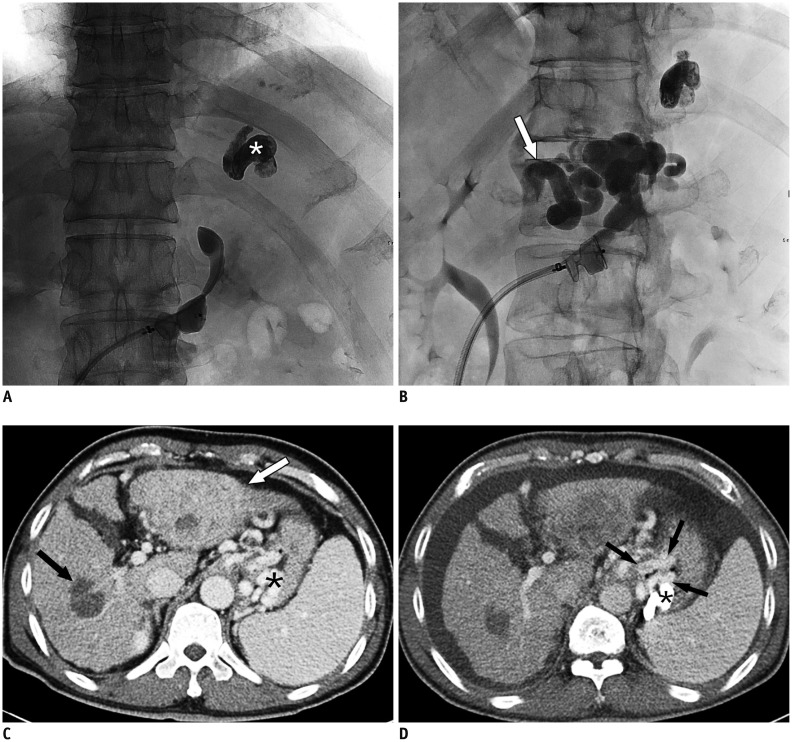
Results: Technical success (complete occlusion of the efferent shunt and complete filling of gastric varix [GV] with a gelfoam slurry) was achieved in 18 of 19 (94.7%) patients. The embolic materials could not reach the GV in 1 patient who had endoscopic glue injection before our procedure. The clinical success rate (no recurrence of gastric variceal bleeding) was the same because the technically failed patient showed recurrent bleeding later. Acute complications included fever (n = 2), fever and hypotension (n = 2; one diagnosed adrenal insufficiency), and transient microscopic hematuria (n = 3). Ten patients underwent follow-up endoscopy; all exhibited GV improvement, except 2 without endoscopic change. Five patients exhibited aggravated EV, and 2 of them had a bleeding event. Laboratory findings were significantly improved after PARTO.
Conclusion: PARTO is technically feasible, safe, and effective for gastric variceal hemorrhage in patients with portal hypertension.
Keywords: BRTO; Variceal bleeding; Vascular Plug.
Figures
Similar articles
-
Vascular Plug Assisted Retrograde Transvenous Obliteration (PARTO) for Gastric Varix Bleeding Patients in the Emergent Clinical Setting.Yonsei Med J. 2016 Jul;57(4):973-9. doi: 10.3349/ymj.2016.57.4.973. Yonsei Med J. 2016. PMID: 27189294 Free PMC article.
-
Gastric varices and hepatic encephalopathy: treatment with vascular plug and gelatin sponge-assisted retrograde transvenous obliteration--a primary report.Radiology. 2013 Jul;268(1):281-7. doi: 10.1148/radiol.13122102. Epub 2013 Mar 12. Radiology. 2013. PMID: 23481167
-
Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Varices: The Role of Intra-Procedural Cone-Beam Computed Tomography.Korean J Radiol. 2018 Mar-Apr;19(2):223-229. doi: 10.3348/kjr.2018.19.2.223. Epub 2018 Feb 22. Korean J Radiol. 2018. PMID: 29520179 Free PMC article.
-
Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Duodenal Variceal Bleeding - A Case Report and Literature Review.Korean J Gastroenterol. 2023 Dec 25;82(6):295-299. doi: 10.4166/kjg.2023.105. Korean J Gastroenterol. 2023. PMID: 38129999 Review.
-
Modified Balloon-Occluded Retrograde Transvenous Obliteration (BRTO) Techniques for the Treatment of Gastric Varices: Vascular Plug-Assisted Retrograde Transvenous Obliteration (PARTO)/Coil-Assisted Retrograde Transvenous Obliteration (CARTO)/Balloon-Occluded Antegrade Transvenous Obliteration (BATO).Cardiovasc Intervent Radiol. 2018 Jun;41(6):835-847. doi: 10.1007/s00270-018-1896-1. Epub 2018 Feb 7. Cardiovasc Intervent Radiol. 2018. PMID: 29417267 Review.
Cited by
-
Combined Balloon-, Plug- and Coil-assisted Retrograde Transvenous Obliteration of Multiple Portosystemic Shunts to Treat Recurrent Hepatic Encephalopathy: A Case Report.J Clin Exp Hepatol. 2020 Jul-Aug;10(4):402-406. doi: 10.1016/j.jceh.2019.12.002. Epub 2019 Dec 26. J Clin Exp Hepatol. 2020. PMID: 32655241 Free PMC article.
-
Combined approach for embolization of otherwise unmanageable gastric varices.Ann Gastroenterol. 2021 Jul-Aug;34(4):510-515. doi: 10.20524/aog.2021.0616. Epub 2021 Mar 23. Ann Gastroenterol. 2021. PMID: 34276189 Free PMC article.
-
Evolution of Retrograde Transvenous Obliteration Techniques.Semin Intervent Radiol. 2018 Aug;35(3):185-193. doi: 10.1055/s-0038-1660796. Epub 2018 Aug 6. Semin Intervent Radiol. 2018. PMID: 30087521 Free PMC article. Review.
-
Response to Yang et al.Am J Gastroenterol. 2018 Dec;113(12):1902-1903. doi: 10.1038/s41395-018-0385-0. Epub 2018 Oct 25. Am J Gastroenterol. 2018. PMID: 30361624 Free PMC article. No abstract available.
-
The combination of balloon-assisted antegrade transvenous obliteration and transjugular intrahepatic portosystemic shunt for the management of cardiofundal varices hemorrhage.Eur J Gastroenterol Hepatol. 2020 May;32(5):656-662. doi: 10.1097/MEG.0000000000001705. Eur J Gastroenterol Hepatol. 2020. PMID: 32175982 Free PMC article.
References
-
- de Franchis R, Primignani M. Natural history of portal hypertension in patients with cirrhosis. Clin Liver Dis. 2001;5:645–663. - PubMed
-
- Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992;16:1343–1349. - PubMed
-
- Lee CH, Lee JH, Choi YS, Paik SW, Sinn DH, Lee CY, et al. [Natural history of gastric varices and risk factors for bleeding] Korean J Hepatol. 2008;14:331–341. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
