

doi: 10.3348/kjr.2016.17.2.245.
Epub 2016 Mar 2.
Sonographic Findings of Common Musculoskeletal Diseases in Patients with Diabetes Mellitus
Affiliations
- PMID: 26957910
- PMCID: PMC4781764
- DOI: 10.3348/kjr.2016.17.2.245
Item in Clipboard
Sonographic Findings of Common Musculoskeletal Diseases in Patients with Diabetes Mellitus
Korean J Radiol.
2016 Mar-Apr.
Abstract
Diabetes mellitus (DM) can accompany many musculoskeletal (MSK) diseases. It is difficult to distinguish the DM-related MSK diseases based on clinical symptoms alone. Sonography is frequently used as a first imaging study for these MSK symptoms and is helpful to differentiate the various DM-related MSK diseases. This pictorial essay focuses on sonographic findings of various MSK diseases that can occur in diabetic patients.
Keywords: Diabetes mellitus; Musculoskeletal; Sonography.
Figures
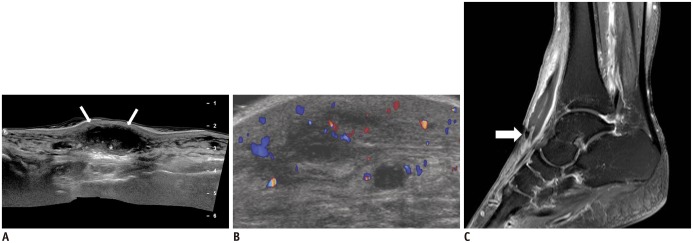
A. Longitudinal sonography scan shows diffuse thickening of subcutaneous tissues with large subcutaneous fluid collection (arrows) filled with echogenic material (asterisk). B. Transverse color Doppler sonography scan shows increased vascularity surrounding multiloculated, hypoechoic fluid collection. Streptococcus viridans was cultured from fluid obtained with sonography-guided aspiration. C. Sagittal enhanced T1-weighted fat-suppressed image shows subcutaneous fluid collection with rim-like enhancement. Drain tube is inserted at fluid collection (arrow). Surrounding edema without involvement of deep soft tissue or bony structure is noted.
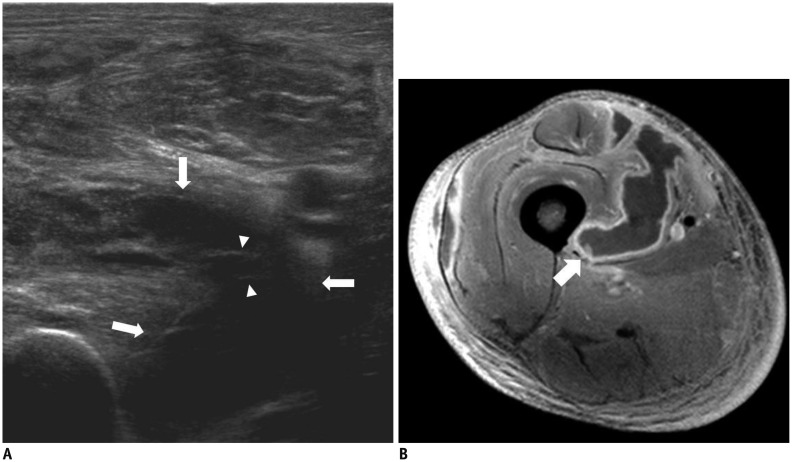
A. Transverse sonography scan of medial thigh shows fluid collection (arrows) with echogenic septa (arrowheads) within vastus medialis muscle. Diffuse edema of adjacent muscles and subcutaneous layer are also noted. B. Axial enhanced T1-weighted fat-suppressed image shows few fluid collections with rim-like enhancement within vastus medialis (arrow), vastus lateralis, and rectus femoris.
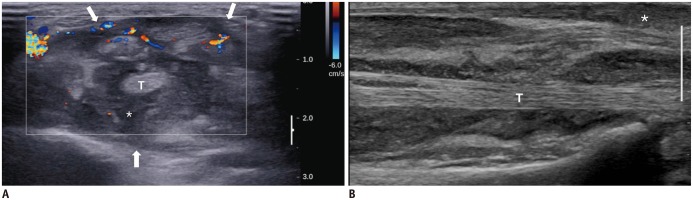
A. Transverse color Doppler sonography scan at distal radioulnar joint level shows distended flexor tendon sheath (arrows) filled with echogenic debris (asterisk) and hypervascularity. Tendons are mildly thickened. B. Longitudinal sonography scan reveals subcutaneous extension of echogenic debris (asterisk), suggesting ruptured tendon sheath. T = tendon
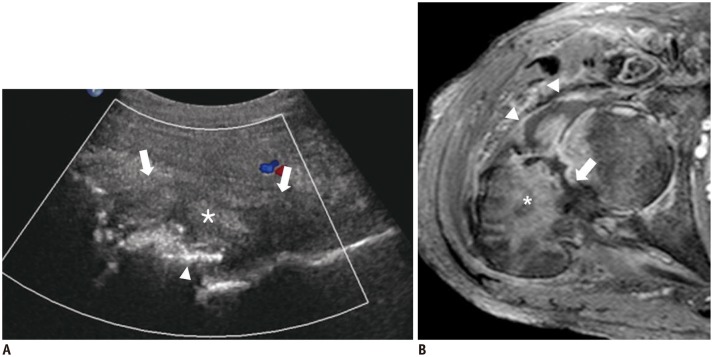
A. Longitudinal sonography scan of anterior aspect of right hip joint shows joint distension (arrows), bone destruction (arrowhead), and fluid with echogenic debris (asterisk) with adjacent soft tissue edema. B. Axial enhanced T1-weighted fat-suppressed image shows septic arthritis of right hip and osteomyelitis (asterisk) with pathologic fracture of femur (arrow). Joint fluid and irregular synovial enhancement (arrowheads) are seen.
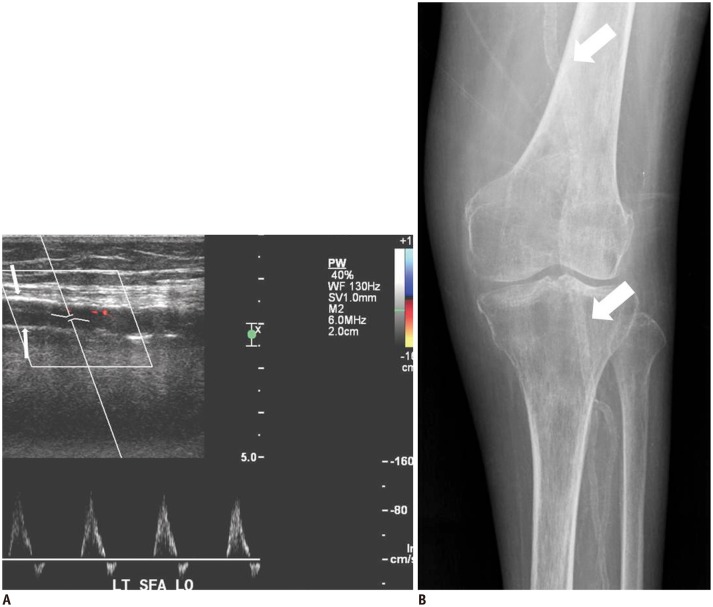
A. Longitudinal sonography scan of superficial femoral artery shows continuous echogenic lines (arrows) in vessel wall without luminal narrowing. Doppler flow pattern shows decreased 2nd reversal flow in early diastole and loss of 3rd wave. These findings are suggestive of decreased resistance of distal arteries and arterial stiffness. B. Plain radiography of left knee shows continuous circumferential fine calcification along superficial femoral artery and popliteal tributaries (arrows).
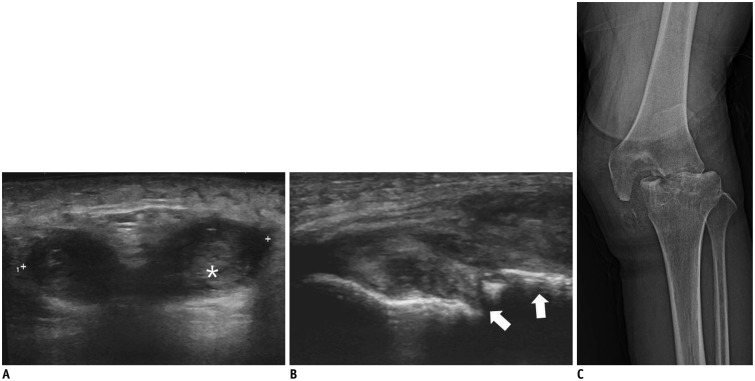
A. Transverse sonography scan of suprapatellar bursa shows large amount of joint effusion filled with echogenic material (asterisk) and diffuse thickening of subcutaneous tissues. B. Longitudinal sonography scan of medial aspect of left knee shows cortical destruction of tibia (arrows) and joint effusion with echogenic materials. C. Plain radiography of left knee shows severe bone destruction with discrete margin, fragmentations, joint subluxation, and soft tissue edema. Serial radiographs (not shown) demonstrate rapid progression of bone destruction.
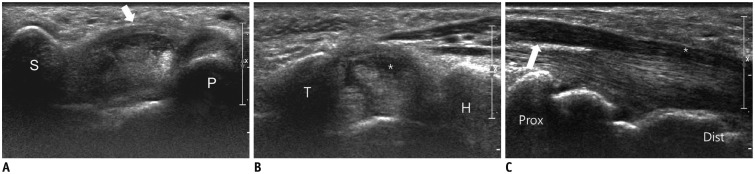
A. Transverse sonography of left wrist scan shows palmar bowing of flexor retinaculum at proximal carpal tunnel level delimited by scaphoid (S) and pisiform (P). Diffuse thickening of flexor retinaculum is noted (arrow). B. Transverse sonography scan shows median nerve flattening (asterisk) at distal carpal tunnel level delimited by hamate (H) and trapezium (T). C. Longitudinal sonography scan shows median nerve flattening (asterisk) at distal (dist) carpal tunnel level and median nerve swelling (arrow) at distal radius level (prox). Surgical release of carpal tunnel was performed because of non-responsiveness to conservative management.
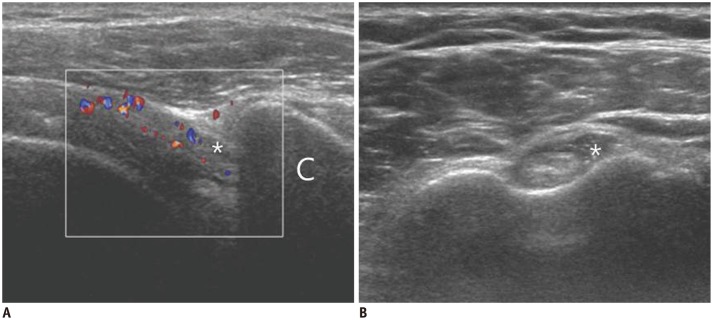
A. Transverse color Doppler sonography scan shows thickening of cuff interval structures with increased vascularity (asterisk). Dynamic sonography scan of right shoulder shows marked limitation of sliding movement of supraspinatus tendon beneath acromion during lateral passive elevation of arm (not visualized in this figure). B. Transverse sonography scan shows distension of biceps long head tendon sheath (asterisk) with joint fluid collection. C = coracoid process
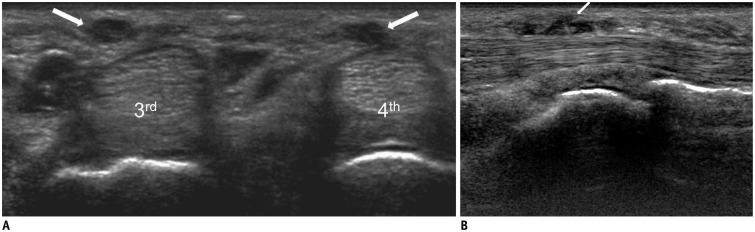
A. Transverse sonography scans shows hypoechoic nodular lesions (arrows) in subcutaneous fat layer of right palm at 3rd and 4th metacarpal head level, suggesting nodular thickening of palmar fascia. B. On longitudinal sonography scan, subcutaneous cord (arrow) at distal crease level is contiguous with thickened tendon sheath of 4th flexor digitorum tendon. 3rd = 3rd metacarpal head, 4th = 4th metacarpal head
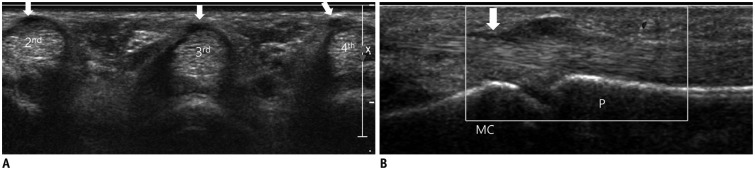
A. Transverse sonography scan shows hypoechoic nodular thickening of first annular pulleys (arrows) at metacarpophalangeal joint level. B. Longitudinal sonography scan shows blurred margin of 2nd flexor digitorum tendon (arrow). 2nd = 2nd flexor digitorum tendon, 3rd = 3rd flexor digitorum tendon, 4th = 4th flexor digitorum tendon, MC = 2nd metacarpal bone, P = 2nd proximal phalanx
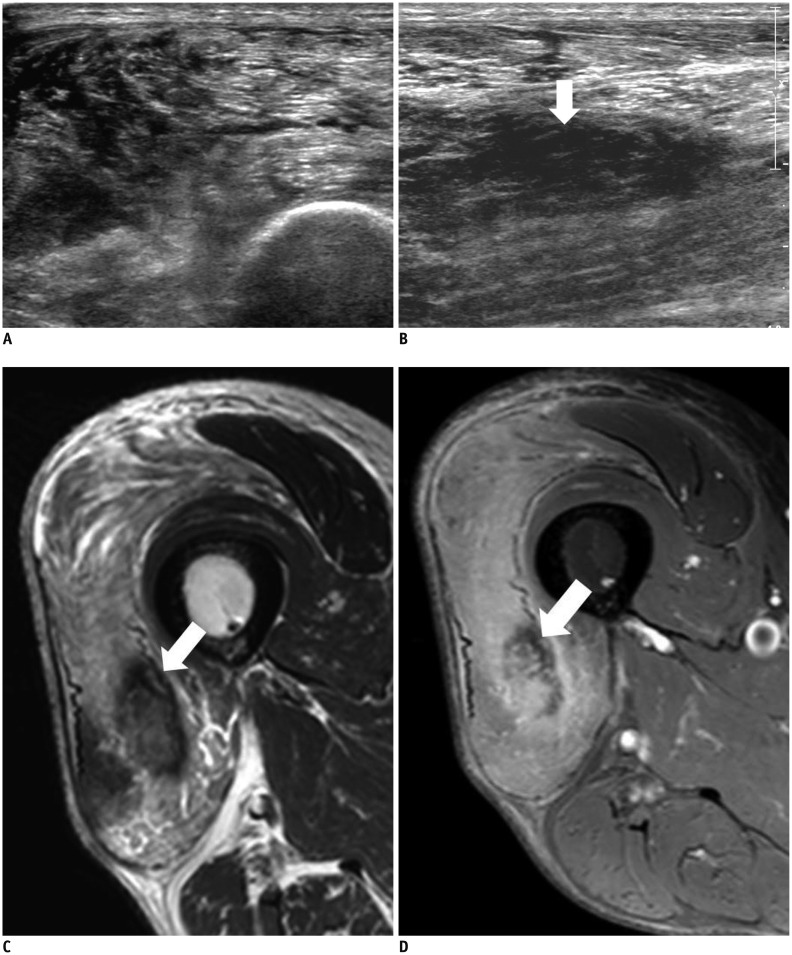
A, B. Transverse (A) and longitudinal (B) sonography scans show heterogeneous echogenicity of right vastus lateralis muscle. On longitudinal scan (B), hypoechoic portion with preservation of echogenic fibrillar pattern of muscle fibers (arrow) is noted. Significant fluid collection is absent. C. Axial T2-weighted MR image shows diffuse edema of right vastus lateralis muscle. Note focal T2 low signal intensity lesion (arrow). D. On axial enhanced T1-weighted fat-suppressed MR image, focal T2 low signal lesion corresponds to lesion with decreased enhancement and surrounding enhancement (arrow).
Similar articles
-
Musculoskeletal infections: ultrasound appearances.Clin Radiol. 2005 Feb;60(2):149-59. doi: 10.1016/j.crad.2004.02.005. Clin Radiol. 2005. PMID: 15664569 Review.
-
Rheumatic-musculoskeletal manifestations in type 2 diabetes mellitus patients in south India.Int J Rheum Dis. 2011 Feb;14(1):55-60. doi: 10.1111/j.1756-185X.2010.01587.x. Epub 2011 Jan 24. Int J Rheum Dis. 2011. PMID: 21303482
-
Beyond ulcers and osteomyelitis: imaging of less common musculoskeletal complications in diabetes mellitus.Br J Radiol. 2018 Jul;91(1088):20170301. doi: 10.1259/bjr.20170301. Epub 2018 Feb 22. Br J Radiol. 2018. PMID: 29419313 Free PMC article. Review.
-
Musculoskeletal manifestations of diabetes mellitus.QJM. 2015 Nov;108(11):853-7. doi: 10.1093/qjmed/hcv106. Epub 2015 May 28. QJM. 2015. PMID: 26025688 Review.
-
Diabetes mellitus-related musculoskeletal disorders: Unveiling the cluster of diseases.Prim Care Diabetes. 2023 Dec;17(6):548-553. doi: 10.1016/j.pcd.2023.08.003. Epub 2023 Aug 27. Prim Care Diabetes. 2023. PMID: 37643934 Review.
Cited by
-
Computed Tomography Imaging Characteristics in the Diagnosis and Assessment of Cellulitis in Patients with Leg Swelling.Medicina (Kaunas). 2025 May 26;61(6):982. doi: 10.3390/medicina61060982. Medicina (Kaunas). 2025. PMID: 40572669 Free PMC article.
-
Imaging for Dupuytren disease: a systematic review of the literature.BMC Musculoskelet Disord. 2019 May 17;20(1):224. doi: 10.1186/s12891-019-2606-0. BMC Musculoskelet Disord. 2019. PMID: 31101038 Free PMC article.
-
The sonographic quantitative assessment of the deltoid muscle to detect type 2 diabetes mellitus: a potential noninvasive and sensitive screening method?BMC Endocr Disord. 2022 Jul 27;22(1):193. doi: 10.1186/s12902-022-01107-2. BMC Endocr Disord. 2022. PMID: 35897066 Free PMC article.
References
-
- Joshi N, Caputo GM, Weitekamp MR, Karchmer AW. Infections in patients with diabetes mellitus. N Engl J Med. 1999;341:1906–1912. - PubMed
-
- Chau CL, Griffith JF. Musculoskeletal infections: ultrasound appearances. Clin Radiol. 2005;60:149–159. - PubMed
-
- Turecki MB, Taljanovic MS, Stubbs AY, Graham AR, Holden DA, Hunter TB, et al. Imaging of musculoskeletal soft tissue infections. Skeletal Radiol. 2010;39:957–971. - PubMed
-
- Patel SR, Olenginski TP, Perruquet JL, Harrington TM. Pyomyositis: clinical features and predisposing conditions. J Rheumatol. 1997;24:1734–1738. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
