

Immunochemical Assays and Nucleic-Acid Detection Techniques for Clinical Diagnosis of Prostate Cancer
- PMID: 26958088
- PMCID: PMC4780128
- DOI: 10.7150/jca.13821
Immunochemical Assays and Nucleic-Acid Detection Techniques for Clinical Diagnosis of Prostate Cancer
Abstract
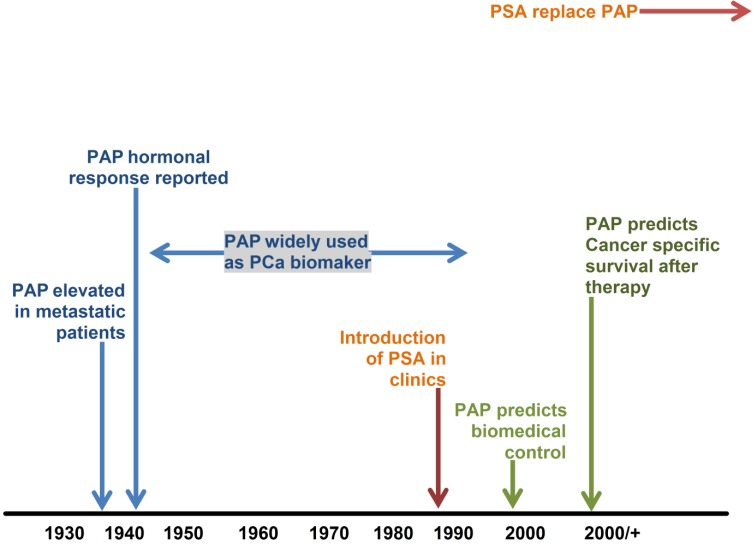
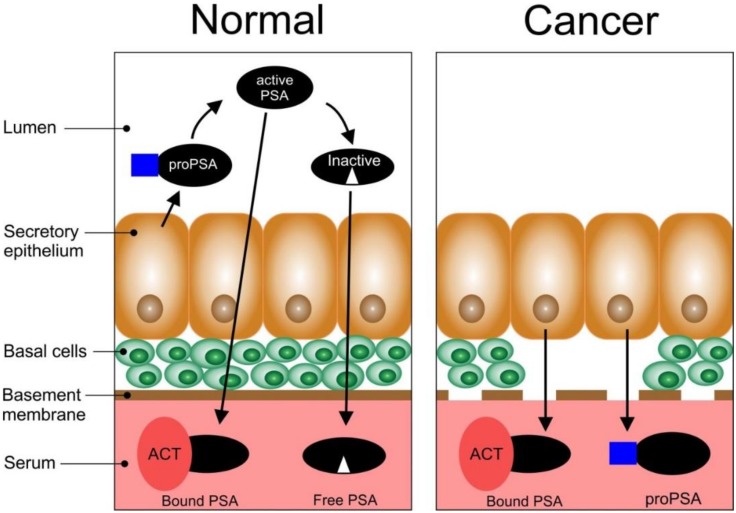
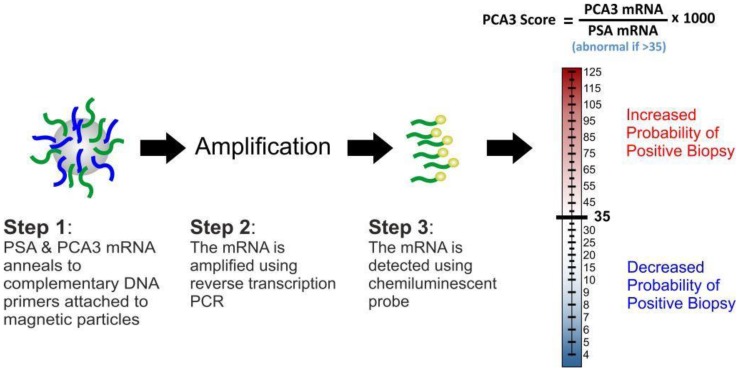
Prostate cancer (PCa) is a significant cause of morbidity and mortality and the most common cancer in men in Europe, North America, and some parts of Africa. The established methods for detecting PCa are normally based on tests using Prostate Specific Antigen (PSA) in blood, Prostate cancer antigen 3 (PCA3) in urine and tissue Alpha-methylacyl-CoA racemase (AMACR) as tumour markers in patient samples. Prior to the introduction of PSA in clinics, prostatic acid phosphatase (PAP) was the most widely used biomarker. An early diagnosis of PCa through the detection of these biomarkers requires the availability of simple, reliable, cost-effective and robust techniques. Immunoassays and nucleic acid detection techniques have experienced unprecedented growth in recent years and seem to be the most promising analytical tools. This growth has been driven in part by the surge in demand for near-patient-testing systems in clinical diagnosis. This article reviews immunochemical assays, and nucleic-acid detection techniques that have been used to clinically diagnose PCa.
Keywords: Biopsy; Clinical Diagnosis; Immunoassays; PAP; PSA.; Prostate Cancer.
Conflict of interest statement
Conflict of interest: The authors declare no conflict of interest.
Figures
Similar articles
-
Prostate Cancer Diagnosis Using Urine Sediment Analysis-Based α-Methylacyl-CoA Racemase Score: A Single-Center Experience.Cancer Control. 2019 Jan-Dec;26(1):1073274819887697. doi: 10.1177/1073274819887697. Cancer Control. 2019. PMID: 31793344 Free PMC article.
-
Identification of Clinically Significant Prostate Cancer by Combined PCA3 and AMACR mRNA Detection in Urine Samples.Res Rep Urol. 2020 Sep 17;12:403-413. doi: 10.2147/RRU.S262310. eCollection 2020. Res Rep Urol. 2020. PMID: 32984088 Free PMC article.
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Urinary Prostate Cancer Antigen 3 as a Tumour Marker: Biochemical and Clinical Aspects.Adv Exp Med Biol. 2015;867:277-89. doi: 10.1007/978-94-017-7215-0_17. Adv Exp Med Biol. 2015. PMID: 26530372 Review.
-
Contemporary role of prostate cancer antigen 3 in the management of prostate cancer.Eur Urol. 2011 Nov;60(5):1045-54. doi: 10.1016/j.eururo.2011.08.003. Epub 2011 Aug 25. Eur Urol. 2011. PMID: 21871709 Review.
Cited by
-
Inflammation Thread Runs across Medical Laboratory Specialities.Mediators Inflamm. 2016;2016:4121837. doi: 10.1155/2016/4121837. Epub 2016 Jul 14. Mediators Inflamm. 2016. PMID: 27493451 Free PMC article. Review.
-
Prostate Cancer Diagnosis Using Urine Sediment Analysis-Based α-Methylacyl-CoA Racemase Score: A Single-Center Experience.Cancer Control. 2019 Jan-Dec;26(1):1073274819887697. doi: 10.1177/1073274819887697. Cancer Control. 2019. PMID: 31793344 Free PMC article.
-
Identification of Clinically Significant Prostate Cancer by Combined PCA3 and AMACR mRNA Detection in Urine Samples.Res Rep Urol. 2020 Sep 17;12:403-413. doi: 10.2147/RRU.S262310. eCollection 2020. Res Rep Urol. 2020. PMID: 32984088 Free PMC article.
References
-
- Ferlay J, Shin HR, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917. - PubMed
-
- Population Reference Bureau. World Population Data Sheet in 2014.
-
- GLOBOCAN. Prostate cancer, estimated incidence, mortality and prevalence worldwide in 2012. International Agency for Research on Cancer (World Health Organisation)
-
- Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas DB. Cancer incidence in five continents. International Agency for Research on Cancer (World Health Organisation); 1997.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
