

Perfusion and Oxygenation of Random Advancement Skin Flaps Depend More on the Length and Thickness of the Flap Than on the Width to Length Ratio
- PMID: 26958105
- PMCID: PMC4764830
Perfusion and Oxygenation of Random Advancement Skin Flaps Depend More on the Length and Thickness of the Flap Than on the Width to Length Ratio
Abstract
Objective: The aim was to investigate the relationship between the dimensions (length, width, and thickness) of random advancement skin flaps and retained tissue perfusion and oxygenation.
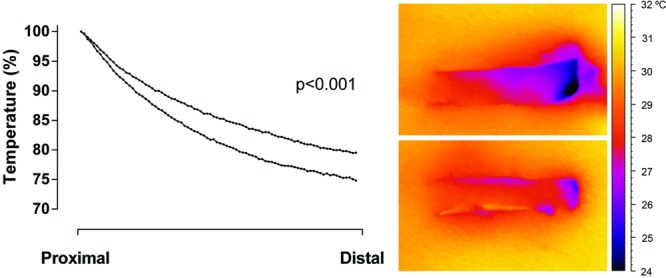
Methods: Flaps were raised on the flanks of pigs. The flaps were either 0.5 or 1.0 cm wide, thin (dissected halfway through the subcutaneous tissue) or thick (dissected down to the muscle fascia). Tissue perfusion was measured by laser Doppler velocimetry, and tissue oxygenation (pO2) was measured using a Licox system, every 0.5 cm along the flaps' length. Tissue temperature was visualized by high-resolution infrared camera.
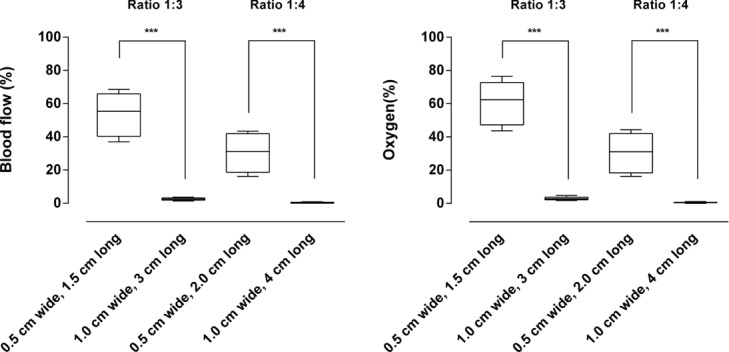
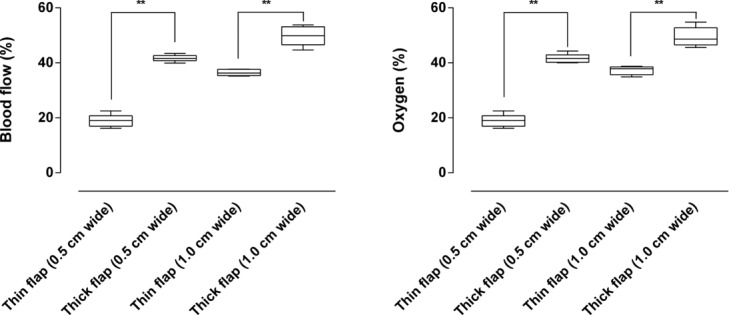
Results: Perfusion and oxygenation decreased gradually from the base to the tip of the flap, reaching approximately 40% of presurgical values (2.0 cm) and approximately 20% (2.5 cm) from the base of the flap. There was virtually no blood flow, nor oxygen tension, 3.0 cm from the base of the flap. The width to length ratio of the flap did not determine blood flow or oxygenation, being approximately 30% in a 0.5 cm wide and 2 cm long flap, and 0% in a 1.0 cm wide and 4 cm long flap, both with a width to length ratio of 1:4. Blood flow and oxygenation were preserved to a greater extent in the thick flaps (∼40%) than in the thin flaps (∼20%), in a 0.5 cm wide and 2 cm long flap.
Conclusions: The dissection of a random advancement flap results in hypoperfusion and oxygenation that cannot be predicted by the width to length ratio but depend on the length and thickness of the flap.
Keywords: blood flow; experimental; oxygenation; perfusion; random flaps.
Figures



Similar articles
-
Forehead flap perfusion monitored by laser speckle contrast imaging: Importance of flap length and thickness.JPRAS Open. 2024 Mar 27;40:222-229. doi: 10.1016/j.jpra.2024.03.006. eCollection 2024 Jun. JPRAS Open. 2024. PMID: 38681530 Free PMC article.
-
Perfusion in Upper Eyelid Flaps: Effects of Rotation and Stretching Measured With Laser Speckle Contrast Imaging in Patients.Ophthalmic Plast Reconstr Surg. 2020 Sep/Oct;36(5):481-484. doi: 10.1097/IOP.0000000000001614. Ophthalmic Plast Reconstr Surg. 2020. PMID: 32049945
-
Evaluation of the Microvascular Blood Flow, Oxygenation, and Survival of Tarsoconjunctival Flaps Following the Modified Hughes Procedure.Ophthalmic Plast Reconstr Surg. 2016 Nov/Dec;32(6):468-472. doi: 10.1097/IOP.0000000000000598. Ophthalmic Plast Reconstr Surg. 2016. PMID: 26669289
-
[Experimental study on the relationship between the ratio of length to width of slender narrow pedicle and random flap survival area in pig].Zhonghua Zheng Xing Wai Ke Za Zhi. 2011 Jan;27(1):40-3. Zhonghua Zheng Xing Wai Ke Za Zhi. 2011. PMID: 21548387 Chinese.
-
Blood Perfusion in Rotational Full-Thickness Lower Eyelid Flaps Measured by Laser Speckle Contrast Imaging.Ophthalmic Plast Reconstr Surg. 2020 Mar/Apr;36(2):148-151. doi: 10.1097/IOP.0000000000001496. Ophthalmic Plast Reconstr Surg. 2020. PMID: 31876674 Free PMC article.
Cited by
-
Blood Perfusion in a Full-Thickness Eyelid Flap, Investigated by Laser Doppler Velocimetry, Laser Speckle Contrast Imaging, and Thermography.Eplasty. 2018 Feb 15;18:e9. eCollection 2018. Eplasty. 2018. PMID: 29520316 Free PMC article.
-
Forehead flap perfusion monitored by laser speckle contrast imaging: Importance of flap length and thickness.JPRAS Open. 2024 Mar 27;40:222-229. doi: 10.1016/j.jpra.2024.03.006. eCollection 2024 Jun. JPRAS Open. 2024. PMID: 38681530 Free PMC article.
-
Random pattern hatchet flap as a reconstructive tool in the treatment of pressure sores: clinical experience with 36 patients.Ann R Coll Surg Engl. 2021 May;103(5):374-379. doi: 10.1308/rcsann.2020.7077. Epub 2021 Mar 19. Ann R Coll Surg Engl. 2021. PMID: 33739158 Free PMC article.
-
Clinical Observation of Subepidermal Vascular Network Flaps in Keloid Patients.Aesthetic Plast Surg. 2022 Aug;46(4):2015-2022. doi: 10.1007/s00266-022-02783-0. Epub 2022 Feb 11. Aesthetic Plast Surg. 2022. PMID: 35149890
-
Therapeutic potential of naringin in improving the survival rate of skin flap: A review.Front Pharmacol. 2023 Mar 2;14:1128147. doi: 10.3389/fphar.2023.1128147. eCollection 2023. Front Pharmacol. 2023. PMID: 36937856 Free PMC article. Review.
References
-
- Gillies HD. Plastic Surgery of the Face Based on Selected Cases of War Injuries of the Face Including Burns, with Original Illustrations. Published 1920. Available at: https://archive.org/search.php?query=creator%3A%22Gillies%2C+H.+D.+%28Ha...
-
- Milton SH. Pedicled skin-flaps: the fallacy of the length:width ratio. Br J Surg. 1970;57:502–8. - PubMed
-
- Daniel RK, Williams HB. The free transfer of skin flaps by microvascular anastomoses. An experimental study and a reappraisal. Plast Reconstr Surg. 1973;52:16–31. - PubMed
-
- Stranc MF, Sowa MG, Abdulrauf B, Mantsch HH. Assessment of tissue viability using near-infrared spectroscopy. Br J Plast Surg. 1998;51:210–7. - PubMed
LinkOut - more resources
Full Text Sources