

Incidence of Hospitalization for Respiratory Syncytial Virus Infection amongst Children in Ontario, Canada: A Population-Based Study Using Validated Health Administrative Data
- PMID: 26958849
- PMCID: PMC4784925
- DOI: 10.1371/journal.pone.0150416
Incidence of Hospitalization for Respiratory Syncytial Virus Infection amongst Children in Ontario, Canada: A Population-Based Study Using Validated Health Administrative Data
Abstract
Importance: RSV is a common illness among young children that causes significant morbidity and health care costs.
Objective: Routinely collected health administrative data can be used to track disease incidence, explore risk factors and conduct health services research. Due to potential for misclassification bias, the accuracy of data-elements should be validated prior to use. The objectives of this study were to validate an algorithm to accurately identify pediatric cases of hospitalized respiratory syncytial virus (RSV) from within Ontario's health administrative data, estimate annual incidence of hospitalization due to RSV and report the prevalence of major risk factors within hospitalized patients.
Study design and setting: A retrospective chart review was performed to establish a reference-standard cohort of children from the Ottawa region admitted to the Children's Hospital of Eastern Ontario (CHEO) for RSV-related disease in 2010 and 2011. Chart review data was linked to Ontario's administrative data and used to evaluate the diagnostic accuracy of algorithms of RSV-related ICD-10 codes within provincial hospitalization and emergency department databases. Age- and sex-standardized incidence was calculated over time, with trends in incidence assessed using Poisson regression.
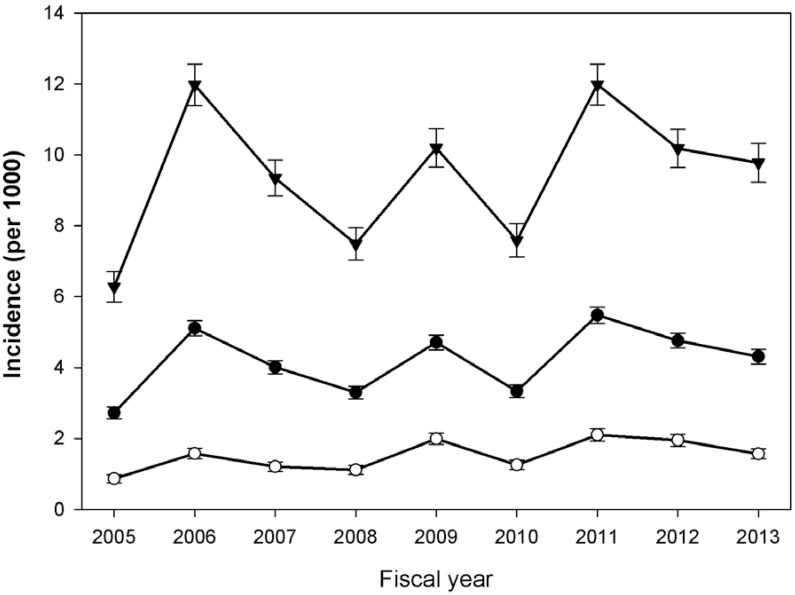
Results: From a total of 1411 admissions, chart review identified 327 children hospitalized for laboratory confirmed RSV-related disease. Following linkage to administrative data and restriction to first admissions, there were 289 RSV patients in the reference-standard cohort. The best algorithm, based on hospitalization data, resulted in sensitivity 97.9% (95%CI: 95.5-99.2%), specificity 99.6% (95%CI: 98.2-99.8%), PPV 96.9% (95%CI: 94.2-98.6%), NPV 99.4% (95%CI: 99.4-99.9%). Incidence of hospitalized RSV in Ontario from 2005-2012 was 10.2 per 1000 children under 1 year and 4.8 per 1000 children aged 1 to 3 years. During the surveillance period, there was no identifiable increasing or decreasing linear trend in the incidence of hospitalized RSV, hospital length of stay and PICU admission rates. Among the Ontario RSV cohort, 16.3% had one or more major risk factors, with a decreasing trend observed over time.
Conclusion: Children hospitalized for RSV-related disease can be accurately identified within population-based health administrative data. RSV is a major public health concern and incidence has not changed over time, suggesting a lack of progress in prevention.
Conflict of interest statement
Figures

References
-
- Nair H, Verma VR, Theodoratou E, Zgaga L, Huda T, Simões EA, et al. An evaluation of the emerging interventions against Respiratory Syncytial Virus (RSV)-associated acute lower respiratory infections in children. BMC public health. 2011;11 Suppl 3(Suppl 3):S30–S. 10.1186/1471-2458-11-S3-S30 - DOI - PMC - PubMed
-
- Glezen WP, Taber LH, Frank AL, Kasel JA. Risk of primary infection and reinfection with respiratory syncytial virus. American Journal of Diseases of children (1960). 1986;140(6):543–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
