

CD4+/CD8+ ratio, age, and risk of serious noncommunicable diseases in HIV-infected adults on antiretroviral therapy
- PMID: 26959354
- PMCID: PMC4785819
- DOI: 10.1097/QAD.0000000000001005
CD4+/CD8+ ratio, age, and risk of serious noncommunicable diseases in HIV-infected adults on antiretroviral therapy
Abstract
Objective: In virologically suppressed HIV-infected adults, noncommunicable diseases (NCDs) have been associated with immune senescence and low CD4/CD8 lymphocyte ratio. Age differences in the relationship between CD4/CD8 ratio and NCDs have not been described.
Design: Observational cohort study.
Methods: We assessed CD4/CD8 ratio and incident NCDs (cardiovascular, cancer, liver, and renal diseases) in HIV-infected adults started on antiretroviral therapy between 1998 and 2012. Study inclusion began once patients maintained virologic suppression for 12 months (defined as baseline). We examined age and baseline CD4/CD8 ratio and used Cox proportional hazard models to assess baseline CD4/CD8 ratio and NCDs.
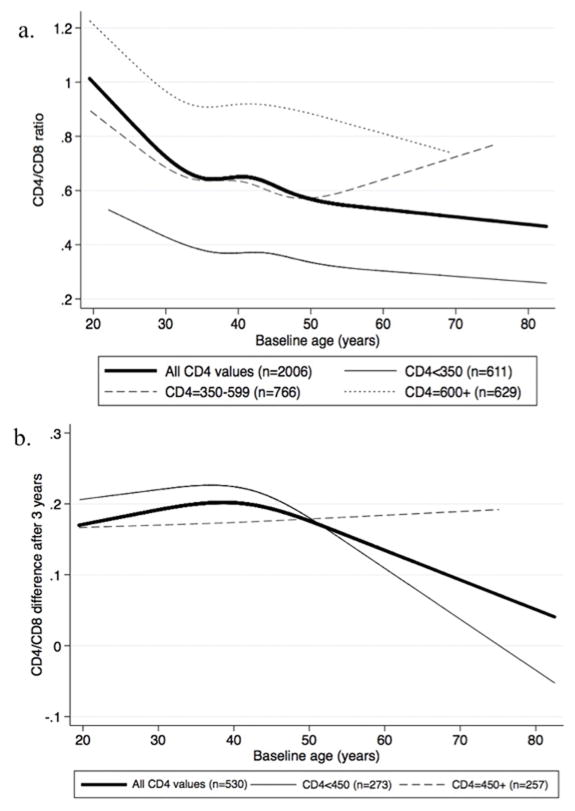
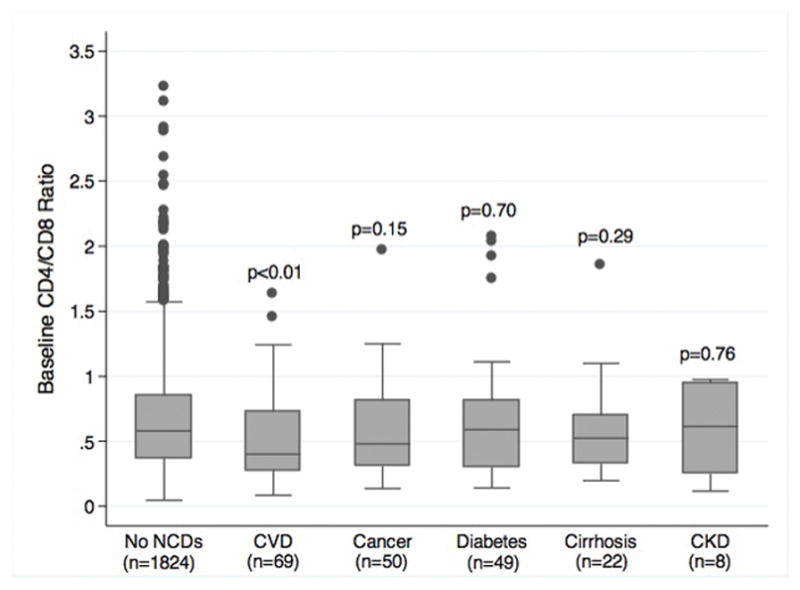
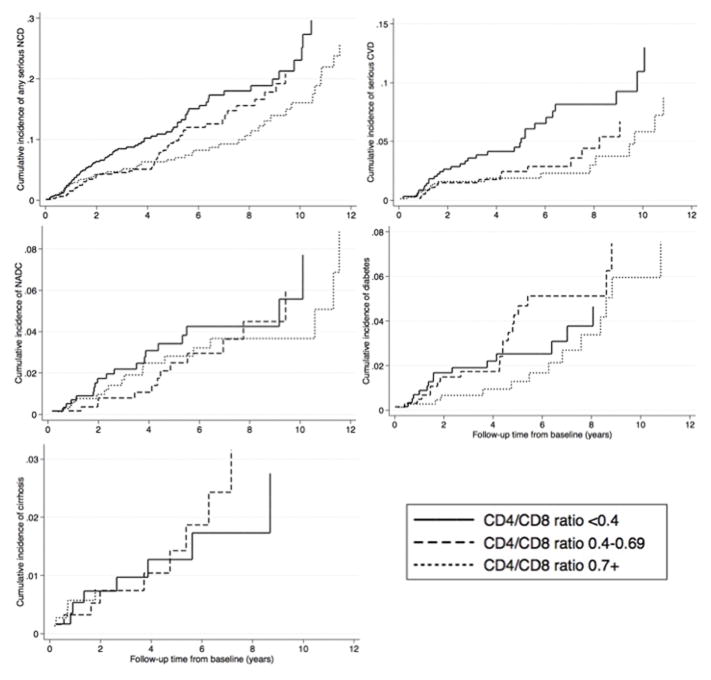
Results: This study included 2006 patients. Low baseline CD4/CD8 ratio was associated with older age, male sex, and low CD4 lymphocyte counts. In models adjusting for CD4 lymphocyte count, CD4/CD8 ratio was inversely associated with age (P < 0.01). Among all patients, 182 had incident NCDs, including 46 with coronary artery disease (CAD) events. CD4/CD8 ratio was inversely associated with risk of CAD events [adjusted HR per 0.1 increase in CD4/CD8 ratio = 0.87, 95% confidence interval (CI): 0.76-0.99, P = 0.03]. This association was driven by those under age 50 years (adjusted HR 0.83 [0.70-0.97], P = 0.02) vs. those over age 50 years (adjusted HR = 0.96 [0.79-1.18], P = 0.71). CD4/CD8 ratio was not significantly associated with incident noncardiac NCDs.
Conclusions: Higher CD4/CD8 ratio after 1 year of HIV virologic suppression was independently predictive of decreased CAD risk, particularly among younger adults. Advanced immune senescence may contribute to CAD events in younger HIV patients on antiretroviral therapy.
Figures
References
-
- Palella FJ, Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. - PubMed
-
- Palella FJ, Jr, Baker RK, Moorman AC, Chmiel JS, Wood KC, Brooks JT, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34. - PubMed
-
- McComsey GA, Kitch D, Sax PE, Tierney C, Jahed NC, Melbourne K, et al. Associations of inflammatory markers with AIDS and non-AIDS clinical events after initiation of antiretroviral therapy: AIDS clinical trials group A5224s, a substudy of ACTG A5202. J Acquir Immune Defic Syndr. 2014;65:167–174. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
