

Continuous glucose monitoring in preterm infants: evaluation by a modified Clarke error grid
- PMID: 26960676
- PMCID: PMC4784331
- DOI: 10.1186/s13052-016-0236-9
Continuous glucose monitoring in preterm infants: evaluation by a modified Clarke error grid
Abstract
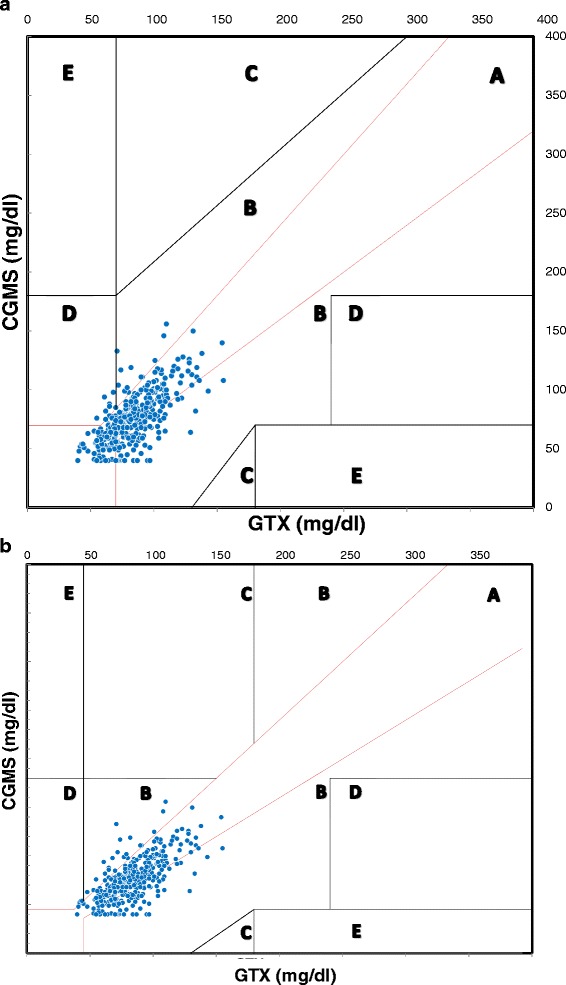
Background: Continuous glucose monitoring using subcutaneous sensors has been validated in adults and children with diabetes, and was found to be useful in the management of glucose control. We aimed to assess feasibility and reliability of a new continuous glucose monitoring system (CGMS) in a population of preterm neonates using a Clarke error grid (CEG) specifically modified for preterm infants.
Methods: Preterm infants were recruited within 24 h from delivery. A subcutaneous sensor connected to a CGMS was inserted and maintained for 6 days. Data collected from CGMS were compared with data obtained using a glucometer. Management of the infants followed standard protocols and was not influenced by CGMS readings.
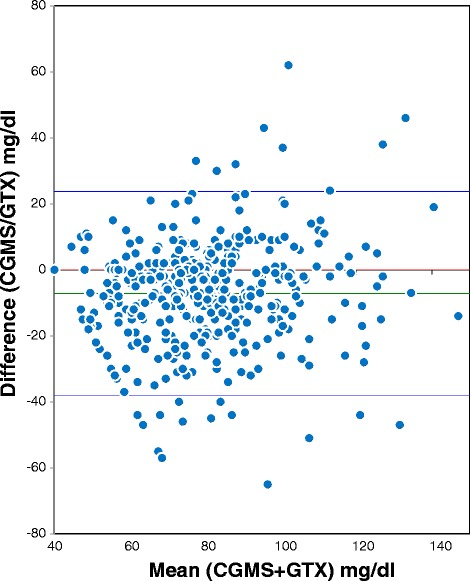
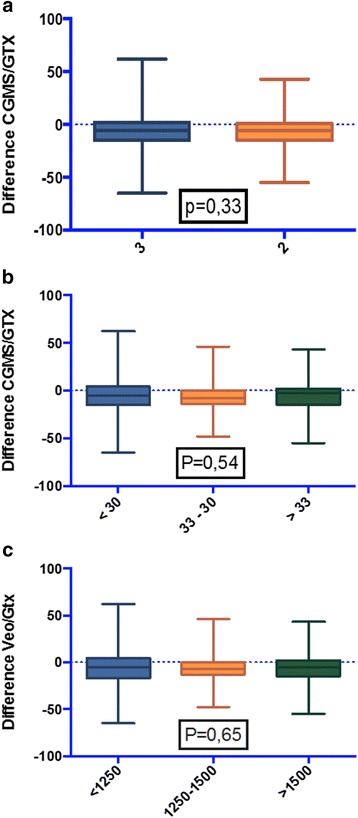
Results: Twenty patients (9 males) were included. Median (range) gestational age was 32 weeks (27-36) and median (range) birth weight was 1350 g (860-3360). Average CGMS recording time was 137 h, for a total of 449 paired glucose levels. CEG and modified CEG criteria for clinical significance were met.
Conclusion: CGMS is a safe and clinically adequate method to estimate glucose levels in preterm infants. As the glucose level can be evaluated in real time, this CGMS could be useful to reduce the number of heel sticks, to observe glycaemic trends and to promptly detect episodes of both hypo- and hyper-glycaemia.
Figures
References
-
- Finberg L. Dangers to infants caused by changes in osmolal concentration. Pediatrics. 1967;40:1031–1034. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
