

Multi-Center, Community-Based Cardiac Implantable Electronic Devices Registry: Population, Device Utilization, and Outcomes
- PMID: 26961369
- PMCID: PMC4943256
- DOI: 10.1161/JAHA.115.002798
Multi-Center, Community-Based Cardiac Implantable Electronic Devices Registry: Population, Device Utilization, and Outcomes
Abstract
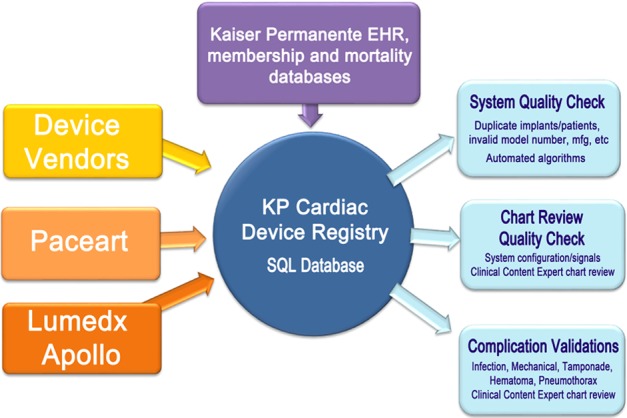
Background: The purpose of this study is to describe key elements, clinical outcomes, and potential uses of the Kaiser Permanente-Cardiac Device Registry.
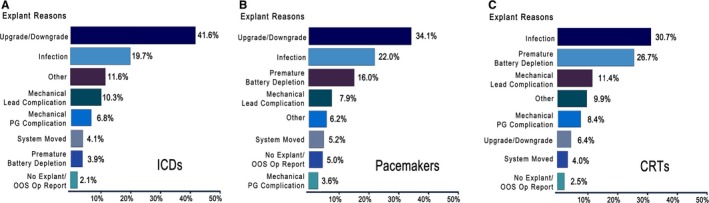
Methods and results: This is a cohort study of implantable cardioverter defibrillators (ICD), pacemakers (PM), and cardiac resynchronization therapy (CRT) devices implanted between January 1, 2007 and December 31, 2013 by ≈400 physicians in 6 US geographical regions. Registry data variables, including patient characteristics, comorbidities, indication for procedures, complications, and revisions, were captured using the healthcare system's electronic medical record. Outcomes were identified using electronic screening algorithms and adjudicated via chart review. There were 11 924 ICDs, 33 519 PMs, 4472 CRTs, and 66 067 leads registered. A higher proportion of devices were implanted in males: 75.1% (ICD), 55.0% (PM), and 66.7% (CRT), with mean patient age 63.2 years (ICD), 75.2 (PM), and 67.2 (CRT). The 30-day postoperative incidence of tamponade, hematoma, and pneumothorax were ≤0.3% (ICD), ≤0.6% (PM), and ≤0.4% (CRT). Device failures requiring revision occurred at a rate of 2.17% for ICDs, 0.85% for PMs, and 4.93% for CRTs, per 100 patient observation years. Superficial infection rates were <0.03% for all devices; deep infection rates were 0.6% (ICD), 0.5% (PM), and 1.0% (CRT). Results were used to monitor vendor-specific variations and were systematically shared with individual regions to address potential variations in outcomes, utilization, and to assist with the management of device recalls.
Conclusions: The Kaiser Permanente-Cardiac Device Registry is a robust tool to monitor postprocedural patient outcomes and postmarket surveillance of implants and potentially change practice patterns.
Keywords: electrophysiology; pacemakers; registries.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures

References
-
- Mond HG, Proclemer A. The 11th world survey of cardiac pacing and implantable cardioverter‐defibrillators: calendar year 2009—a World Society of Arrhythmia's project. Pacing Clin Electrophysiol. 2011;34:1013–1027. - PubMed
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NAM, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL. 2012 ACCF/AHA/HRS focused update incorporated into the ACCF/AHA/HRS 2008 guidelines for device‐based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2013;127:e283–e352. - PubMed
-
- Greenspon AJ, Patel JD, Lau E, Ochoa JA, Frisch DR, Ho RT, Pavri BB, Kurtz SM. Trends in permanent pacemaker implantation in the United States from 1993 to 2009: increasing complexity of patients and procedures. J Am Coll Cardiol. 2012;60:1540–1545. - PubMed
-
- Resnic FS, Normand SL. Postmarketing surveillance of medical devices—filling in the gaps. N Engl J Med. 2012;366:875–877. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
