

Efficacy and Safety of Ceftazidime-Avibactam Plus Metronidazole Versus Meropenem in the Treatment of Complicated Intra-abdominal Infection: Results From a Randomized, Controlled, Double-Blind, Phase 3 Program
- PMID: 26962078
- PMCID: PMC4872289
- DOI: 10.1093/cid/ciw133
Efficacy and Safety of Ceftazidime-Avibactam Plus Metronidazole Versus Meropenem in the Treatment of Complicated Intra-abdominal Infection: Results From a Randomized, Controlled, Double-Blind, Phase 3 Program
Abstract
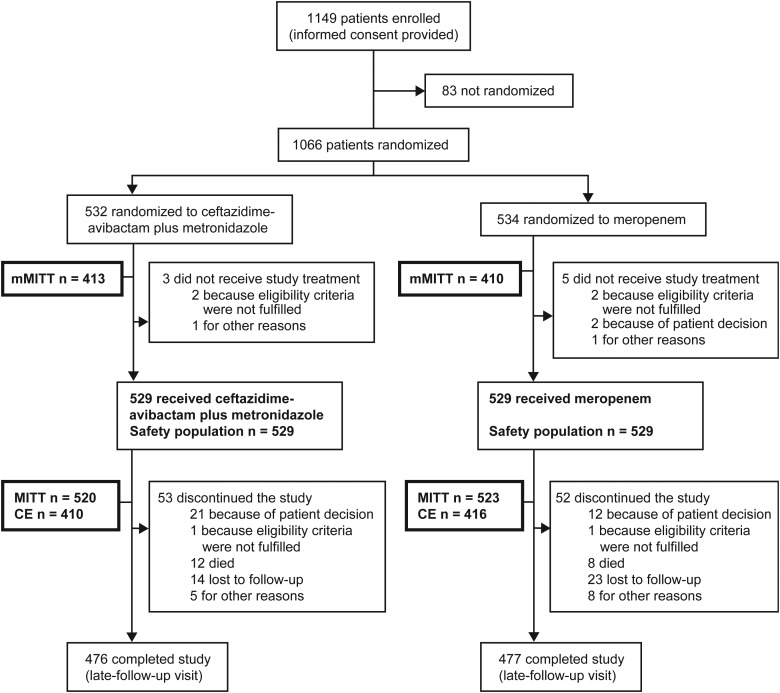
Background: When combined with ceftazidime, the novel non-β-lactam β-lactamase inhibitor avibactam provides a carbapenem alternative against multidrug-resistant infections. Efficacy and safety of ceftazidime-avibactam plus metronidazole were compared with meropenem in 1066 men and women with complicated intra-abdominal infections from 2 identical, randomized, double-blind phase 3 studies (NCT01499290 and NCT01500239).
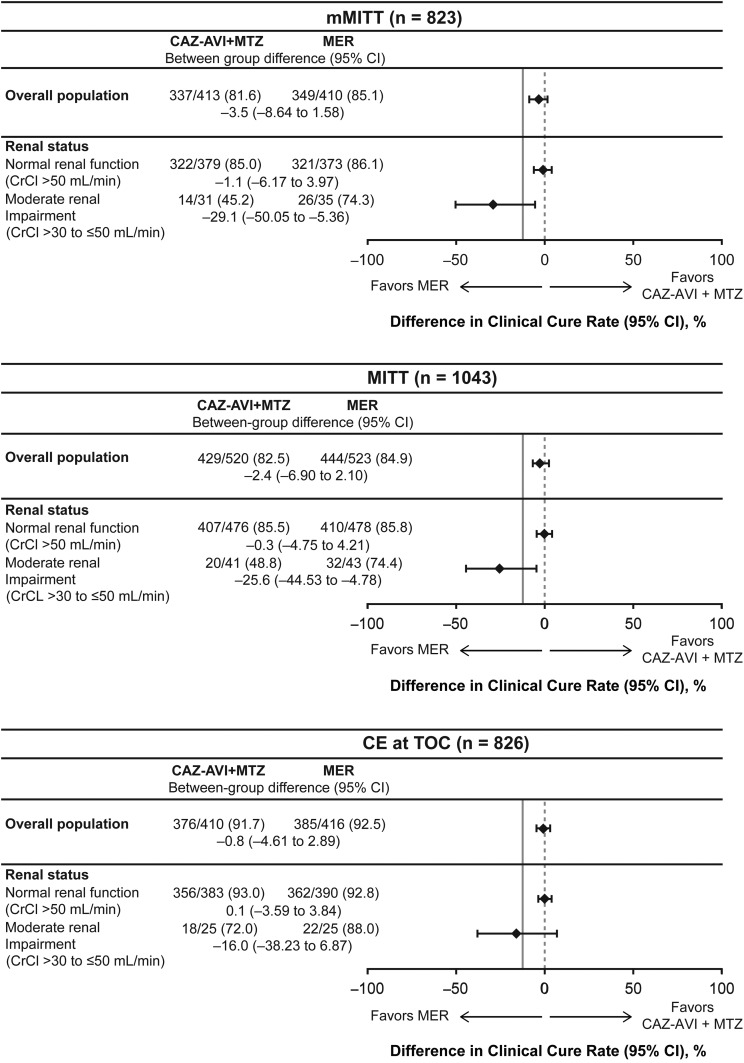
Methods: The primary end point was clinical cure at test-of-cure visit 28-35 days after randomization, assessed by noninferiority of ceftazidime-avibactam plus metronidazole to meropenem in the microbiologically modified intention-to-treat (mMITT) population (in accordance with US Food and Drug Administration guidance), and the modified intention-to-treat and clinically evaluable populations (European Medicines Agency guidance). Noninferiority was considered met if the lower limit of the 95% confidence interval for between-group difference was greater than the prespecified noninferiority margin of -12.5%.
Results: Ceftazidime-avibactam plus metronidazole was noninferior to meropenem across all primary analysis populations. Clinical cure rates with ceftazidime-avibactam plus metronidazole and meropenem, respectively, were as follows: mMITT population, 81.6% and 85.1% (between-group difference, -3.5%; 95% confidence interval -8.64 to 1.58); modified intention-to-treat, 82.5% and 84.9% (-2.4%; -6.90 to 2.10); and clinically evaluable, 91.7% and 92.5% (-0.8%; -4.61 to 2.89). The clinical cure rate with ceftazidime-avibactam plus metronidazole for ceftazidime-resistant infections was comparable to that with meropenem (mMITT population, 83.0% and 85.9%, respectively) and similar to the regimen's own efficacy against ceftazidime-susceptible infections (82.0%). Adverse events were similar between groups.
Conclusions: Ceftazidime-avibactam plus metronidazole was noninferior to meropenem in the treatment of complicated intra-abdominal infections. Efficacy was similar against infections caused by ceftazidime-susceptible and ceftazidime-resistant pathogens. The safety profile of ceftazidime-avibactam plus metronidazole was consistent with that previously observed with ceftazidime alone.
Clinical trials registration: NCT01499290 and NCT01500239.
Keywords: ceftazidime-avibactam plus metronidazole; complicated intra-abdominal infection; meropenem; noninferiority; phase 3.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Nordmann P, Poirel L, Walsh TR, Livermore DM. The emerging NDM carbapenemases. Trends Microbiol 2011; 19:588–95. - PubMed
-
- Kanj SS, Kanafani ZA. Current concepts in antimicrobial therapy against resistant gram-negative organisms: extended-spectrum beta-lactamase-producing Enterobacteriaceae, carbapenem-resistant Enterobacteriaceae, and multidrug-resistant Pseudomonas aeruginosa. Mayo Clin Proc 2011; 86:250–9. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
