

Comparison of the Cytomegalovirus (CMV) Enzyme-Linked Immunosorbent Spot and CMV QuantiFERON Cell-Mediated Immune Assays in CMV-Seropositive and -Seronegative Pregnant and Nonpregnant Women
- PMID: 26962091
- PMCID: PMC4844750
- DOI: 10.1128/JCM.03128-15
Comparison of the Cytomegalovirus (CMV) Enzyme-Linked Immunosorbent Spot and CMV QuantiFERON Cell-Mediated Immune Assays in CMV-Seropositive and -Seronegative Pregnant and Nonpregnant Women
Abstract
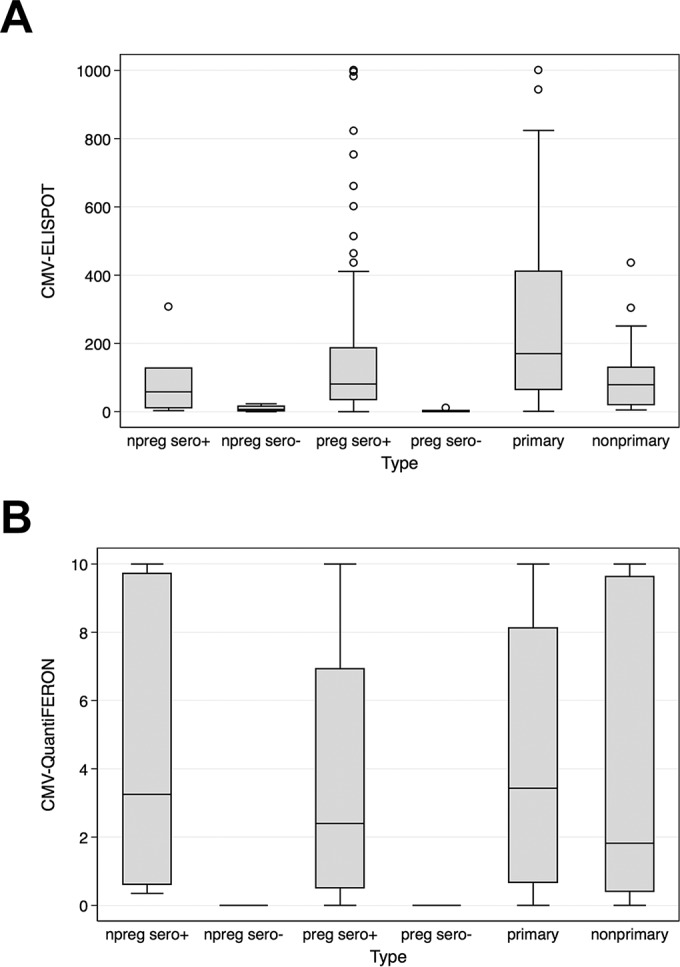
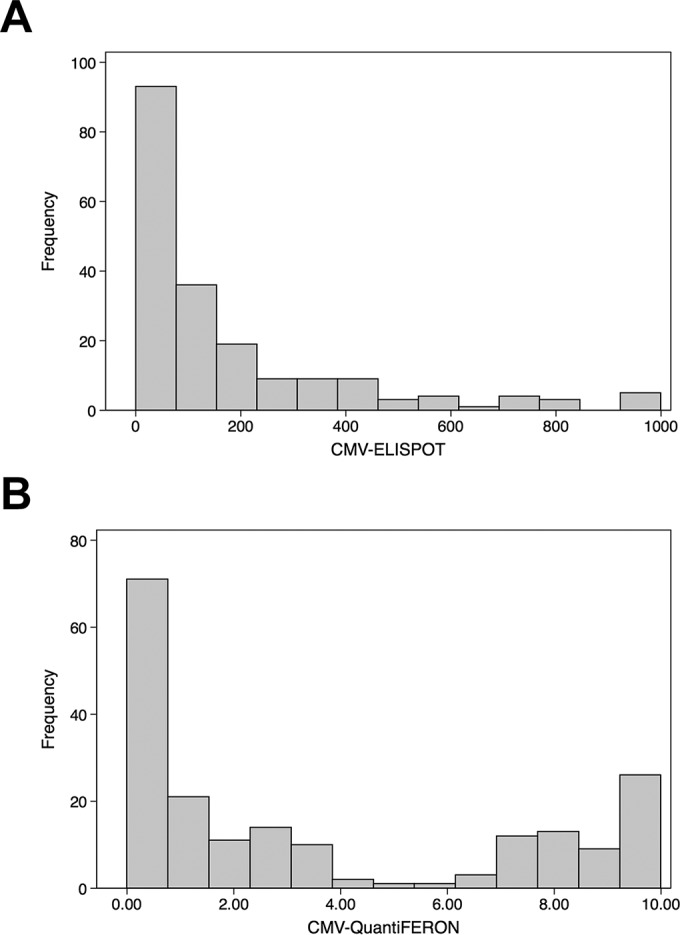
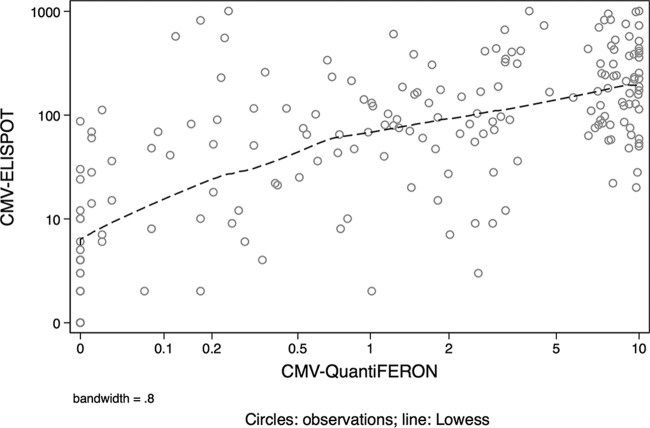
Human cytomegalovirus (CMV) infection is a major cause of congenital infection leading to birth defects and sensorineural anomalies, including deafness. Recently, cell-mediated immunity (CMI) in pregnant women has been shown to correlate with congenital CMV transmission. In this study, two interferon gamma release assays (IGRA), the CMV enzyme-linked immunosorbent spot (ELISPOT) and CMV QuantiFERON assays, detecting CMV-specific CMI were compared. These assays were performed for 80 CMV-infected (57 primarily and 23 nonprimarily) pregnant women and 115 controls, including 89 healthy CMV-seropositive pregnant women without active CMV infection, 15 CMV-seronegative pregnant women, and 11 seropositive or seronegative nonpregnant women. Statistical tests, including frequency distribution analysis, nonparametric Kruskal-Wallis equality-of-populations rank test, Wilcoxon rank sum test for equality on unmatched data, and lowess smoothing local regression, were employed to determine statistical differences between groups and correlation between the assays. The CMV ELISPOT and CMV QuantiFERON assay data were not normally distributed and did not display equal variance. The CMV ELISPOT but not CMV QuantiFERON assay displayed significant higher values for primarily CMV-infected women than for the healthy seropositive pregnant and nonpregnant groups (P = 0.0057 and 0.0379, respectively) and those with nonprimary infections (P = 0.0104). The lowess local regression model comparing the assays on an individual basis showed a value bandwidth of 0.8. Both assays were highly accurate in discriminating CMV-seronegative pregnant women. The CMV ELISPOT assay was more effective than CMV-QuantiFERON in differentiating primary from the nonprimary infections. A substantial degree of variability exists between CMV ELISPOT and CMV QuantiFERON assay results for CMV-seropositive pregnant women.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
