

Colorectal Cancer Screening Based on Age and Gender: A Cost-Effectiveness Analysis
- PMID: 26962772
- PMCID: PMC4998853
- DOI: 10.1097/MD.0000000000002739
Colorectal Cancer Screening Based on Age and Gender: A Cost-Effectiveness Analysis
Abstract
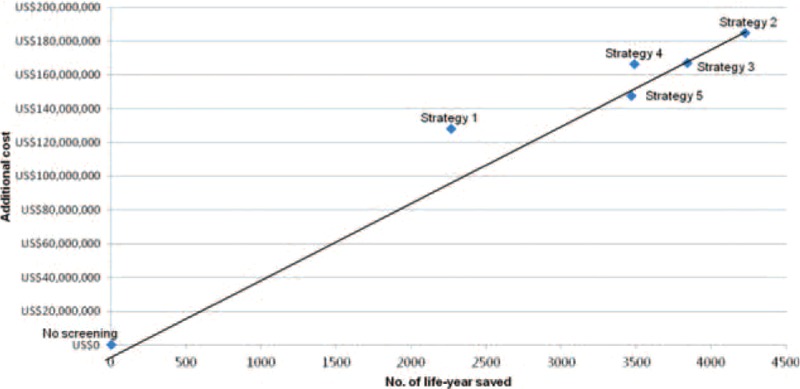
We evaluated whether age- and gender-based colorectal cancer screening is cost-effective.Recent studies in the United States identified age and gender as 2 important variables predicting advanced proximal neoplasia, and that women aged <60 to 70 years were more suited for sigmoidoscopy screening due to their low risk of proximal neoplasia. Yet, quantitative assessment of the incremental benefits, risks, and cost remains to be performed.Primary care screening practice (2008-2015).A Markov modeling was constructed using data from a screening cohort. The following strategies were compared according to the Incremental Cost Effectiveness Ratio (ICER) for 1 life-year saved: flexible sigmoidoscopy (FS) 5 yearly; colonoscopy 10 yearly; FS for each woman at 50- and 55-year old followed by colonoscopy at 60- and 70-year old; FS for each woman at 50-, 55-, 60-, and 65-year old followed by colonoscopy at 70-year old; FS for each woman at 50-, 55-, 60-, 65-, and 70-year old. All male subjects received colonoscopy at 50-, 60-, and 70-year old under strategies 3 to 5.From a hypothetical population of 100,000 asymptomatic subjects, strategy 2 could save the largest number of life-years (4226 vs 2268 to 3841 by other strategies). When compared with no screening, strategy 5 had the lowest ICER (US$42,515), followed by strategy 3 (US$43,517), strategy 2 (US$43,739), strategy 4 (US$47,710), and strategy 1 (US$56,510). Strategy 2 leads to the highest number of bleeding and perforations, and required a prohibitive number of colonoscopy procedures. Strategy 5 remains the most cost-effective when assessed with a wide range of deterministic sensitivity analyses around the base case.From the cost effectiveness analysis, FS for women and colonoscopy for men represent an economically favorable screening strategy. These findings could inform physicians and policy-makers in triaging eligible subjects for risk-based screening, especially in countries with limited colonoscopic resources. Future research should study the acceptability, feasibility, and feasibility of this risk-based strategy in different populations.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- GLOBOCAN 2012 [Internet]. Cancer Fact Sheet. Colorectal Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available from: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx Accessed on 23 September, 2015.
-
- Sung JJY, Lau JYW, Goh KL, et al. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol 2005; 6:871–876. - PubMed
-
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin 2008; 58:130–160. - PubMed
-
- Sung JJ, Ng SC, Chan FK, et al. An updated Asia Pacific consensus recommendations on colorectal cancer screening. Gut 2015; 64:121–132. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
