

Therapeutic Application of Percutaneous Peritoneovenous (Denver) Shunt in Treating Chylous Ascites in Cancer Patients
- PMID: 26965362
- PMCID: PMC5060070
- DOI: 10.1016/j.jvir.2015.12.014
Therapeutic Application of Percutaneous Peritoneovenous (Denver) Shunt in Treating Chylous Ascites in Cancer Patients
Abstract
Purpose: To evaluate the safety and efficacy of percutaneous peritoneovenous shunt (PPVS) placement in treating intractable chylous ascites (CA) in patients with cancer.
Materials and methods: Data from 28 patients with refractory CA treated with PPVS from April 2001 to June 2015 were reviewed. Demographic characteristics, technical success, efficacy, laboratory values, and complications were recorded. Univariate and multivariate logistic regression analysis was performed.
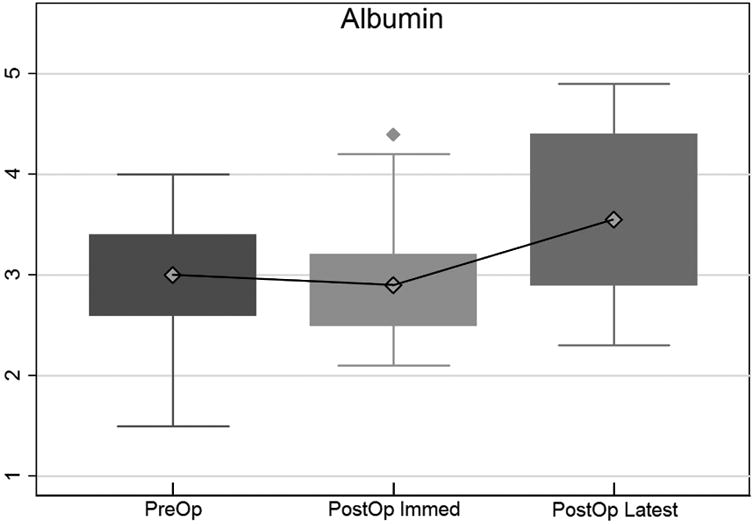
Results: Technical success was 100%, and ascites resolved or symptoms were relieved in 92.3% (26 of 28) of patients. In 13 (46%) patients with urologic malignancies, whose ascites had resulted from retroperitoneal lymph node dissection, the ascites resolved, resulting in shunt removal within 128 days ± 84. The shunt provided palliation of symptoms in 13 of the remaining 15 patients (87%) for a mean duration of 198 days ± 214. Serum albumin levels increased significantly (21.4%) after PPVS placement from a mean of 2.98 g/dL ± 0.64 before the procedure to 3.62 g/dL ± 0.83 (P < .001). The complication rate was 37%, including shunt malfunction/occlusion (22%), venous thrombosis (7%), and subclinical disseminated intravascular coagulopathy (DIC) (7%). Smaller venous limb size (11.5 F) and the presence of peritoneal tumor were associated with a higher rate of shunt malfunction (P < .05). No patient developed overt DIC.
Conclusions: PPVS can safely and effectively treat CA in patients with cancer, resulting in significant improvement in serum albumin in addition to palliation of symptoms.
Copyright © 2016 SIR. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Treatment of Chylous Ascites with Peritoneovenous Shunt (Denver Shunt) following Retroperitoneal Lymph Node Dissection in Patients with Urological Malignancies: Update of Efficacy and Predictors of Complications.J Urol. 2020 Oct;204(4):818-823. doi: 10.1097/JU.0000000000001121. Epub 2020 May 5. J Urol. 2020. PMID: 32364837 Free PMC article.
-
Management of refractory chylous ascites with peritoneovenous shunts.J Vasc Surg Venous Lymphat Disord. 2017 Jul;5(4):538-546. doi: 10.1016/j.jvsv.2017.03.011. Epub 2017 May 9. J Vasc Surg Venous Lymphat Disord. 2017. PMID: 28623993
-
Therapeutic results of Denver percutaneous peritoneovenous shunt in cancer patients with malignant ascites.J Cancer Res Ther. 2020 Dec;16(Supplement):S95-S98. doi: 10.4103/jcrt.JCRT_606_18. J Cancer Res Ther. 2020. PMID: 33380660
-
Denver peritoneovenous shunts for the management of malignant ascites: a review of the literature in the post LeVeen Era.Am Surg. 2011 Aug;77(8):1070-5. doi: 10.1177/000313481107700830. Am Surg. 2011. PMID: 21944526 Review.
-
Management of malignant ascites.Surg Gynecol Obstet. 1984 Oct;159(4):397-412. Surg Gynecol Obstet. 1984. PMID: 6207599 Review.
Cited by
-
Complementary Role of Intervention Radiology in Palliative Care in Oncology Setting.Indian J Palliat Care. 2019 Jul-Sep;25(3):462-467. doi: 10.4103/IJPC.IJPC_24_19. Indian J Palliat Care. 2019. PMID: 31413465 Free PMC article.
-
Quality of life improves after palliative placement of percutaneous tunneled drainage catheter for refractory ascites in prospective study of patients with end-stage cancer.Palliat Support Care. 2019 Dec;17(6):677-685. doi: 10.1017/S1478951519000051. Palliat Support Care. 2019. PMID: 30880658 Free PMC article.
-
Biomarker-guided strategy for Denver peritoneovenous shunts in refractory ascites: a retrospective single-center study.Langenbecks Arch Surg. 2025 Apr 23;410(1):140. doi: 10.1007/s00423-025-03710-y. Langenbecks Arch Surg. 2025. PMID: 40266319 Free PMC article.
-
Milking the System: Dietary Therapy of Post-nephrectomy Chylous Ascites.Dig Dis Sci. 2019 May;64(5):1133-1137. doi: 10.1007/s10620-019-05611-9. Dig Dis Sci. 2019. PMID: 30949904 No abstract available.
-
Treatment of Chylous Ascites with Peritoneovenous Shunt (Denver Shunt) following Retroperitoneal Lymph Node Dissection in Patients with Urological Malignancies: Update of Efficacy and Predictors of Complications.J Urol. 2020 Oct;204(4):818-823. doi: 10.1097/JU.0000000000001121. Epub 2020 May 5. J Urol. 2020. PMID: 32364837 Free PMC article.
References
-
- Evans JG, Spiess PE, Kamat AM, Wood CG, Hernandez M, Pettaway CA, Dinney CP, et al. Chylous ascites after post-chemotherapy retroperitoneal lymph node dissection: review of the M. D. Anderson experience. J Urol. 2006;176:1463–1467. - PubMed
-
- White MA, Agle SC, Padia RK, Zervos EE. Denver peritoneovenous shunts for the management of malignant ascites: a review of the literature in the post LeVeen Era. Am Surg. 2011;77:1070–1075. - PubMed
-
- Sarazin WG, Sauter KE. Chylous ascites following resection of a ruptured abdominal aneurysm. Treatment with a peritoneovenous shunt. Arch Surg. 1986;121:246–247. - PubMed
-
- Fleisher HL, 3rd, Oren JW, Sumner DS. Chylous ascites after abdominal aortic aneurysmectomy: successful management with a peritoneovenous shunt. J Vasc Surg. 1987;6:403–407. - PubMed
-
- Boyd WD, McPhail NV, Barber GC. Chylous ascites following abdominal aortic aneurysmectomy: surgical management with a peritoneovenous shunt. J Cardiovasc Surg (Torino) 1989;30:627–629. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
