

The placental membrane microbiome is altered among subjects with spontaneous preterm birth with and without chorioamnionitis
- PMID: 26965447
- PMCID: PMC4909356
- DOI: 10.1016/j.ajog.2016.01.193
The placental membrane microbiome is altered among subjects with spontaneous preterm birth with and without chorioamnionitis
Abstract
Background: Preterm birth (PTB) is a leading cause of neonatal morbidity and mortality and is not uncommonly associated with chorioamnionitis. We recently have demonstrated that the placenta harbors a unique microbiome with similar flora to the oral community. We also have shown an association of these placental microbiota with PTB, history of antenatal infection, and excess maternal weight gain. On the basis of these previous observations, we hypothesized that the placental membranes would retain a microbiome community that would vary in association with preterm birth and chorioamnionitis.
Objective: In the current study, we aimed to examine the differences in the placental membrane microbiome in association with PTB in both the presence and absence of chorioamnionitis and/or funisitis using state-of-the-science whole-genome shotgun metagenomics.
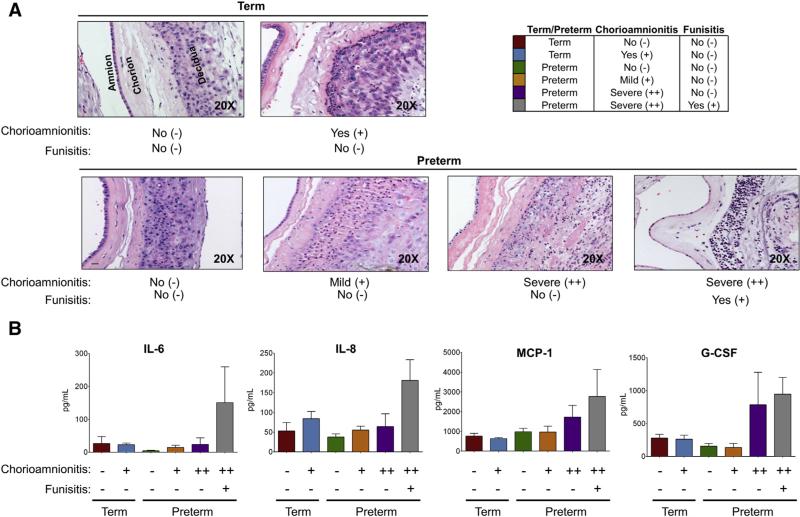
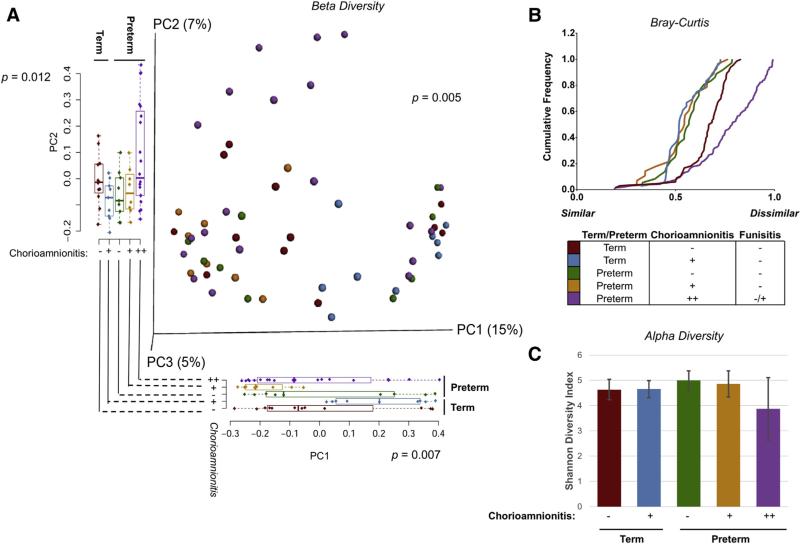
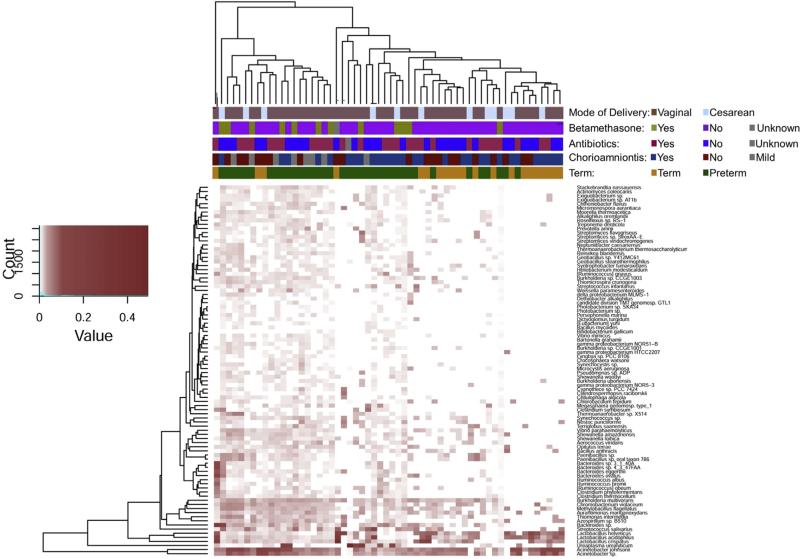
Study design: This was a cross-sectional analysis with 6 nested spontaneous birth cohorts (n = 9-15 subjects/cohort): Term gestations without chorioamnionitis, term with chorioamnionitis, preterm without chorioamnionitis, preterm with mild chorioamnionitis, preterm with severe chorioamnionitis, and preterm with chorioamnionitis and funisitis. Histologic analysis was performed with Redline's criteria, and inflammatory cytokines were analyzed in the cord blood. DNA from placental membranes was extracted from sterile swabs collected at delivery, and whole-genome shotgun sequencing was performed on the Illumina HiSeq platform. Filtered microbial DNA sequences were annotated and analyzed with MG-RAST (ie, Metagenomic Rapid Annotations using Subsystems Technology) and R.
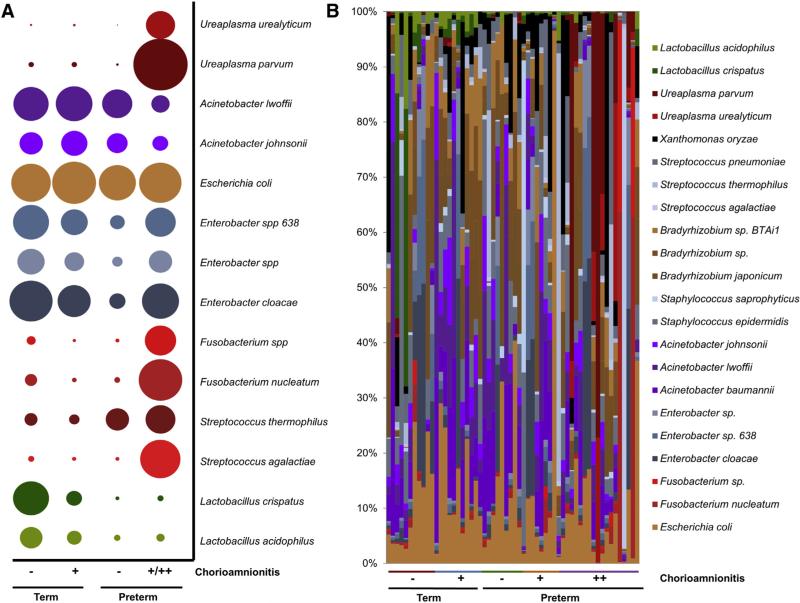
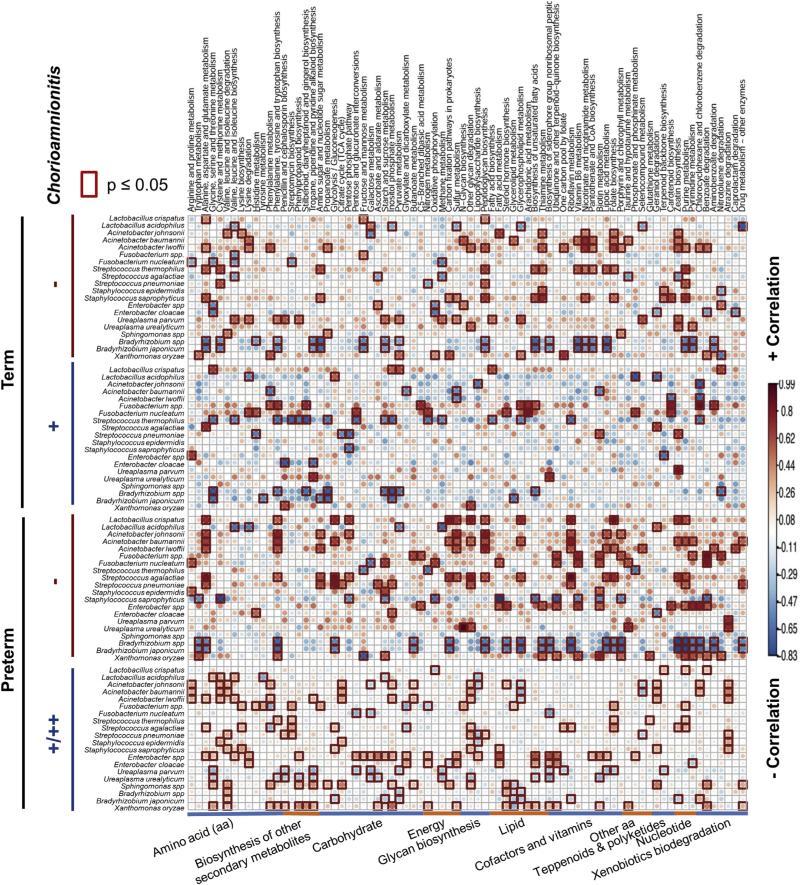
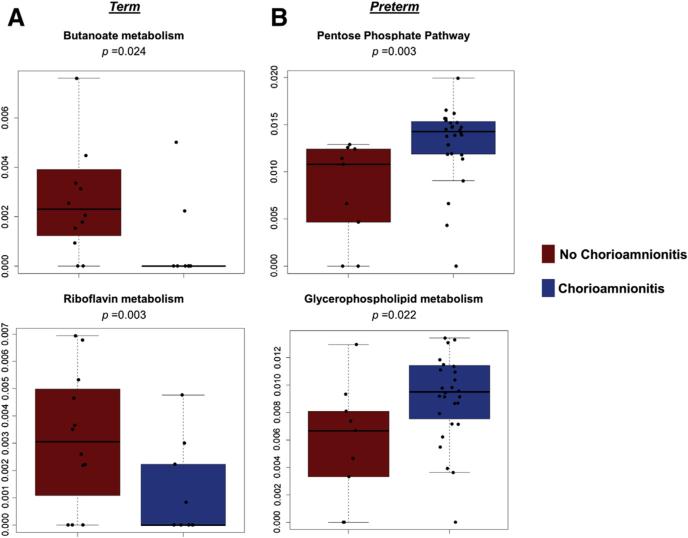
Results: Subjects were assigned to cohorts on the basis of gestational age at delivery and independent scoring of histologic chorioamnionitis. We found that preterm subjects with severe chorioamnionitis and funisitis had increases in cord blood inflammatory cytokines. Of interest, although the placental membrane microbiome was altered in association with severity of histologic chorioamnionitis (permutational multivariate analysis of variance P = .005), there was no observable impact with either betamethasone or antibiotic treatment. In preterm subjects with chorioamnionitis, we found a high abundance of both urogenital and oral commensal bacteria. These alterations in the microbiome were accompanied by significant variation (P < .05) in microbial metabolic pathways important in the glucose-fed pentose phosphate pathway (term subjects), or glycerophopholipid metabolism, and the biosynthesis of the siderophore group nonribosomal peptides (preterm subjects).
Conclusion: Consistent with ours and others previous findings, women who experienced spontaneous PTB harbor placental microbiota that further differed by severity of chorioamnionitis. Integrative metagenomic analysis revealed significant variation in distinct bacterial metabolic pathways, which we speculate may contribute to risk of preterm birth with and without severe chorioamnionitis.
Keywords: chorioamnionitis; funisitis; microbiome; preterm birth; whole-genome shotgun metagenomics.
Copyright © 2016. Published by Elsevier Inc.
Figures
References
-
- Faye-Petersen OM. The placenta in preterm birth. J Clin Pathol. 2008;61:1261–75. - PubMed
-
- Simmons LE, Rubens CE, Darmstadt GL, Gravett MG. Preventing preterm birth and neonatal mortality: exploring the epidemiology, causes, and interventions. Semin Perinatol. 2010;34:408–15. - PubMed
-
- Smulian JC, Shen-Schwarz S, Vintzileos AM, Lake MF, Ananth CV. Clinical chorioamnionitis and histologic placental inflammation. Obstet Gynecol. 1999;94:1000–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
