

Predicting Persistent Left Ventricular Dysfunction Following Myocardial Infarction: The PREDICTS Study
- PMID: 26965540
- PMCID: PMC4854198
- DOI: 10.1016/j.jacc.2015.12.042
Predicting Persistent Left Ventricular Dysfunction Following Myocardial Infarction: The PREDICTS Study
Abstract
Background: Persistent severe left ventricular (LV) systolic dysfunction after myocardial infarction (MI) is associated with increased mortality and is a class I indication for implantation of a cardioverter-defibrillator.
Objectives: This study developed models and assessed independent predictors of LV recovery to >35% and ≥50% after 90-day follow-up in patients presenting with acute MI and severe LV dysfunction.
Methods: Our multicenter prospective observational study enrolled participants with ejection fraction (EF) of ≤35% at the time of MI (n = 231). Predictors for EF recovery to >35% and ≥50% were identified after multivariate modeling and validated in a separate cohort (n = 236).
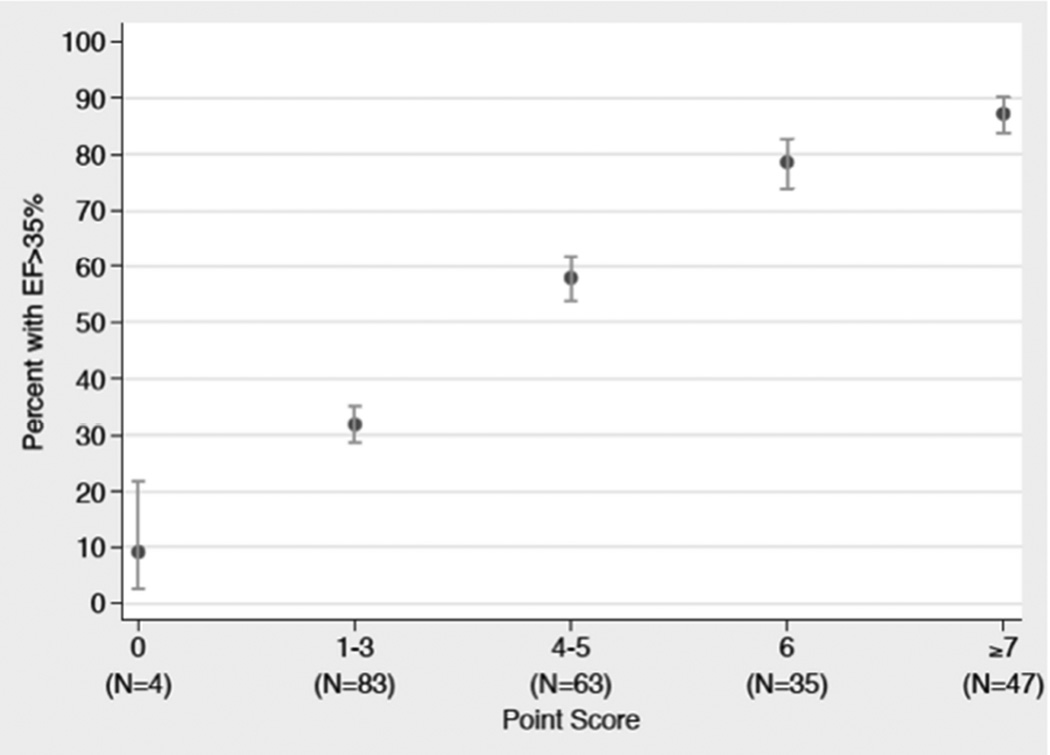
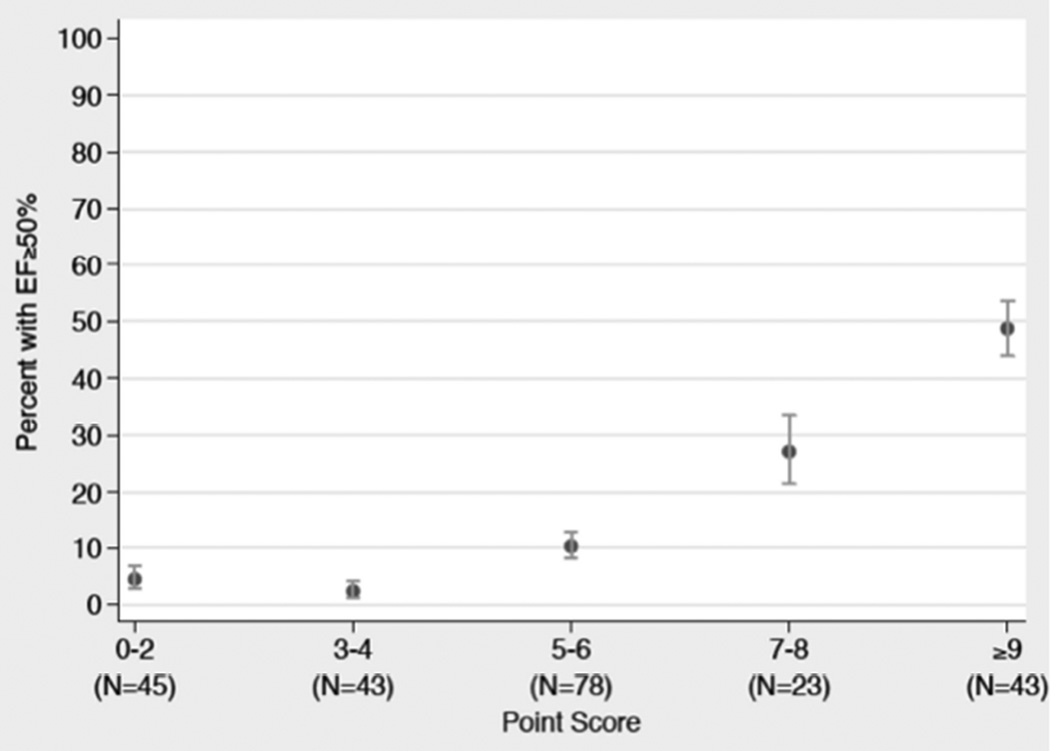
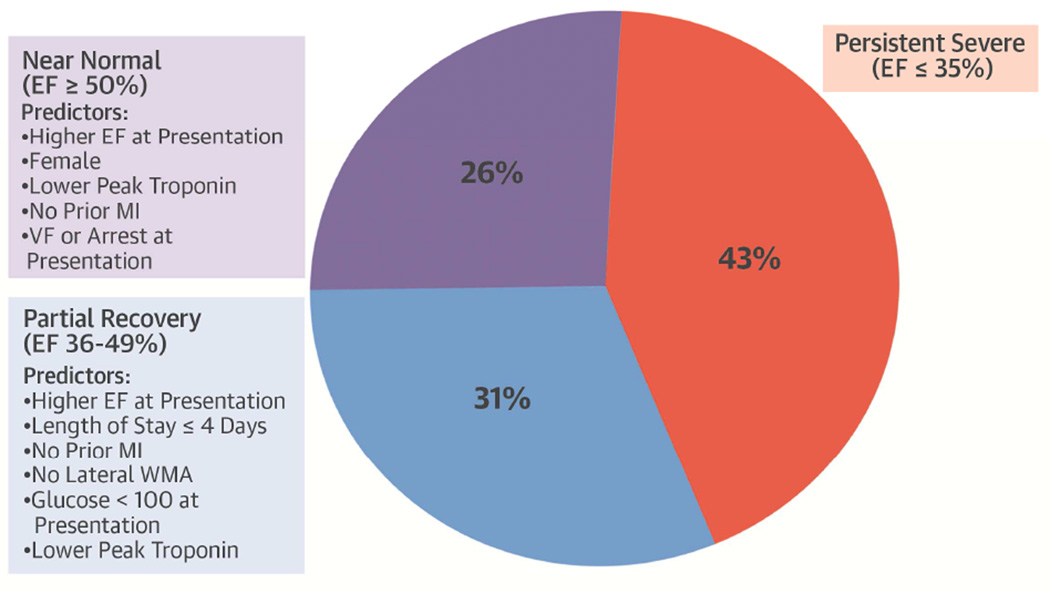
Results: In the PREDICTS (PREDiction of ICd Treatment Study) study, 43% of patients had persistent EF ≤35%, 31% had an EF of 36% to 49%, and 26% had an EF ≥50%. The model that best predicted recovery of EF to >35% included EF at presentation, length of stay, prior MI, lateral wall motion abnormality at presentation, and peak troponin. The model that best predicted recovery of EF to ≥50% included EF at presentation, peak troponin, prior MI, and presentation with ventricular fibrillation or cardiac arrest. After predictors were transformed into point scores, the lowest point scores predicted a 9% and 4% probability of EF recovery to >35% and ≥50%, respectively, whereas profiles with the highest point scores predicted an 87% and 49% probability of EF recovery to >35% and ≥50%, respectively.
Conclusions: In patients with severe systolic dysfunction following acute MI with an EF ≤35%, 57% had EF recovery to >35%. A model using clinical variables present at the time of MI can help predict EF recovery.
Keywords: heart failure; remodeling; risk assessment; ventricular ejection fraction.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Cardiologists Are Accountable to Determine the Need for ICD Therapy After Myocardial Infarction.J Am Coll Cardiol. 2016 Mar 15;67(10):1197-1199. doi: 10.1016/j.jacc.2016.01.021. J Am Coll Cardiol. 2016. PMID: 26965541 No abstract available.
-
Takotsubo-Like State After AMI Complicated by VF or Cardiac Arrest: Misleading Role of First Echocardiogram.J Am Coll Cardiol. 2016 Jul 19;68(3):326-327. doi: 10.1016/j.jacc.2016.04.038. J Am Coll Cardiol. 2016. PMID: 27417015 No abstract available.
References
-
- Epstein AE, DiMarco JP, Ellenbogen KA, et al. 2012 ACCF/AHA/HRS focused update incorporated into the ACCF/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities. J Am Coll Cardiol. 2013;61:e6–e75. - PubMed
-
- Hohnloser SH, Kuck KH, Dorian P, et al. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med. 2004;351:2481–2488. - PubMed
-
- Steinbeck G, Andresen D, Seidl K, et al. Defibrillator implantation early after myocardial infarction. N Engl J Med. 2009;361:1427–1436. - PubMed
-
- Chia S, Senatore F, Raffel OC, et al. Utility of cardiac biomarkers in predicting infarct size, left ventricular function, and clinical outcome after primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. JACC Cardiovasc Interv. 2008;1:415–423. - PubMed
-
- Hackel DB, Reimer KA, Ideker RE, et al. Comparison of enzymatic and anatomic estimates of myocardial infarct size in man. Circulation. 1984;70:824–835. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
