

Vaginal Fibroblastic Cells from Women with Pelvic Organ Prolapse Produce Matrices with Increased Stiffness and Collagen Content
- PMID: 26965792
- PMCID: PMC4786799
- DOI: 10.1038/srep22971
Vaginal Fibroblastic Cells from Women with Pelvic Organ Prolapse Produce Matrices with Increased Stiffness and Collagen Content
Abstract
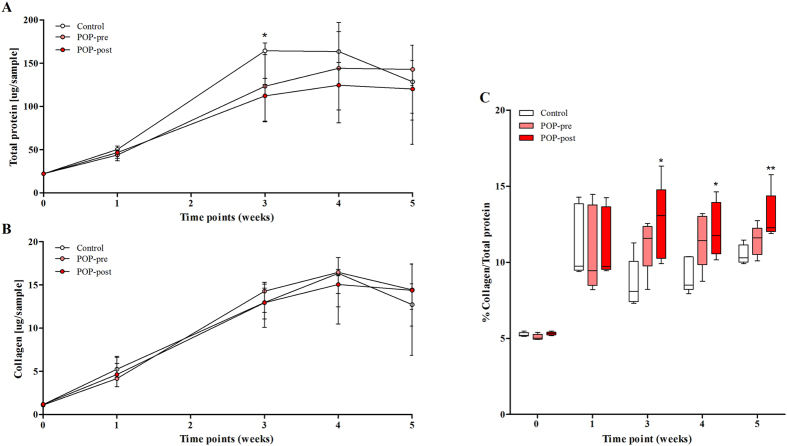
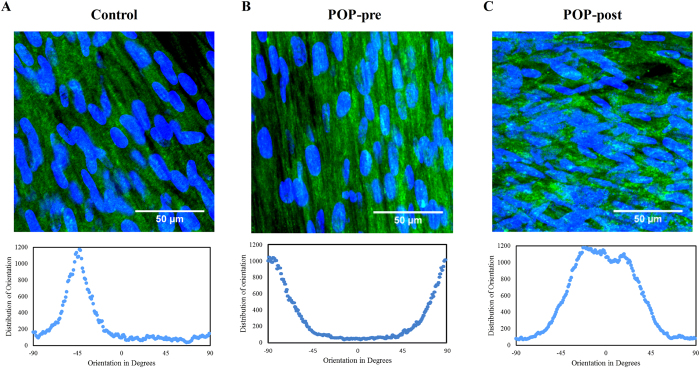
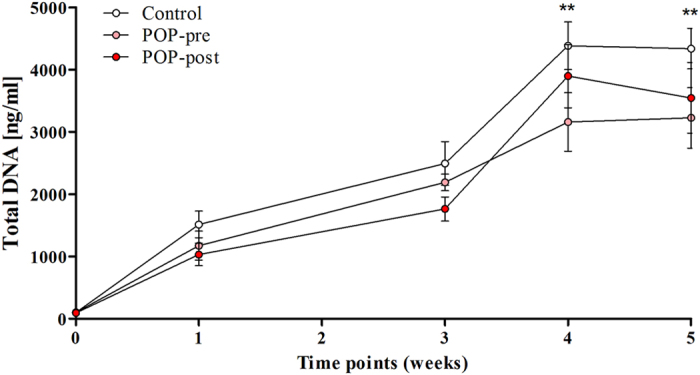
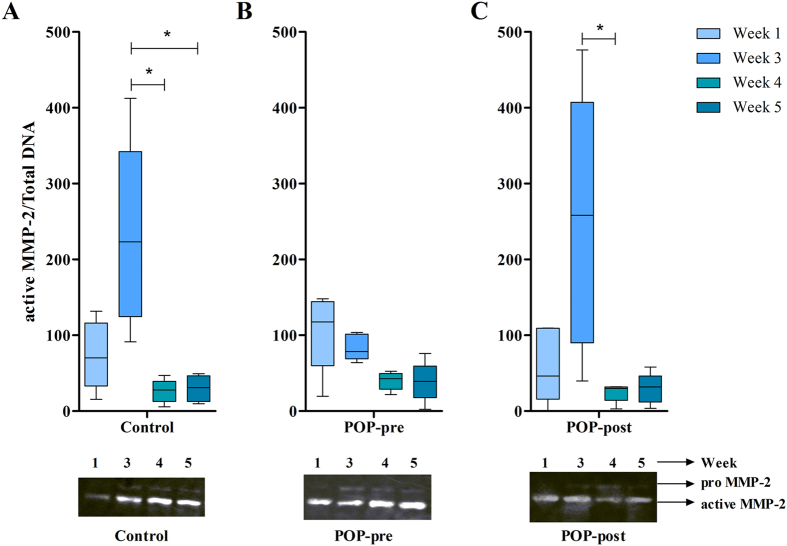
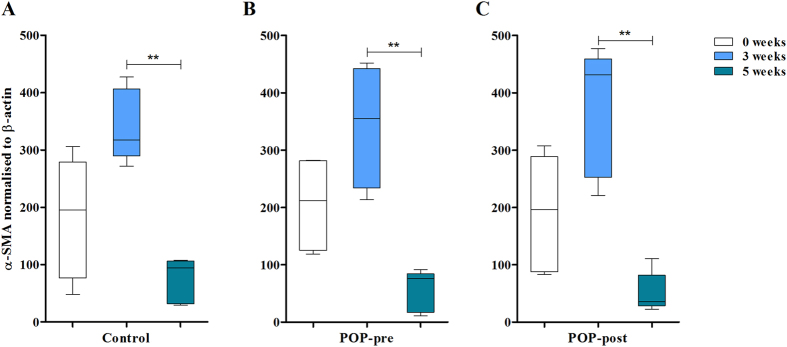
Pelvic organ prolapse (POP) is characterised by the weakening of the pelvic floor support tissues, and often by subsequent prolapse of the bladder outside the body, i.e. cystocele. The bladder is kept in place by the anterior vaginal wall which consists of a dense extracellular matrix rich in collagen content that is maintained and remodelled by fibroblastic cells, i.e. fibroblasts and myofibroblasts. Since altered matrix production influences tissue quality, and myofibroblasts are involved in normal and pathological soft tissue repair processes, we evaluated matrix production of cells derived from pre- and post-menopausal POP and non-POP control anterior vaginal wall tissues. Results showed that cells from postmenopausal POP women deposited matrices with high percentage of collagen fibres with less anisotropic orientation and increased stiffness than those produced by controls. There was a transient increase in myofibroblastic phenotype that was lost after the peak of tissue remodelling. In conclusion, affected fibroblasts from postmenopausal prolapsed tissues produced altered matrices in vitro compared to controls. Such aberrant altered matrix production does not appear to be a consequence of abnormal phenotypical changes towards the myofibroblastic lineage.
Figures
References
-
- Hendrix S. L. et al. Pelvic organ prolapse in women’s health initiative: gravity and gravidity. Am. J. Obstet. Gynecol. 186, 1160–1166 (2002). - PubMed
-
- Jelovsek J. E., Maher C. & Barber M. D. Pelvic organ prolapse. Lancet 396, 1027–1038 (2007). - PubMed
-
- Lensen E. J. M., Withagen M. I. J., Kluivers K. B., Milani A. L. & Vierhout M. E. Surgical treatment of pelvic organ prolapse: a historical review with emphasis on the anterior compartment. Int. Urogynecol. J. 24, 1593–1602 (2013). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
