

Total Pancreatectomy With Islet Autotransplantation Improves Quality of Life in Patients With Refractory Recurrent Acute Pancreatitis
- PMID: 26965843
- PMCID: PMC5538725
- DOI: 10.1016/j.cgh.2016.02.027
Total Pancreatectomy With Islet Autotransplantation Improves Quality of Life in Patients With Refractory Recurrent Acute Pancreatitis
Abstract
Background & aims: Therapeutic options are limited for patients with recurrent acute pancreatitis who have intractable symptoms despite maximal endoscopic and medical treatment, but equivocal or no morphologic or functional evidence of chronic pancreatitis. We performed a prospective observational cohort study to determine the efficacy of total pancreatectomy with islet autotransplantation (TPIAT) for these patients.
Methods: We collected data from all patients undergoing TPIAT at the University of Minnesota from 2007 through 2013; 49 patients (42 female; mean age, 32.8 ± 7.8 years) had a diagnosis of recurrent acute pancreatitis not provoked by intervention, with negative or equivocal findings from nondiagnostic imaging or pancreatic function tests for chronic pancreatitis, and intractable pain between episodes. Data on insulin use, narcotic requirements, pain scores, and health-related quality of life were collected before TPIAT; 3 months, 6 months, and 1 year afterward; and then yearly.
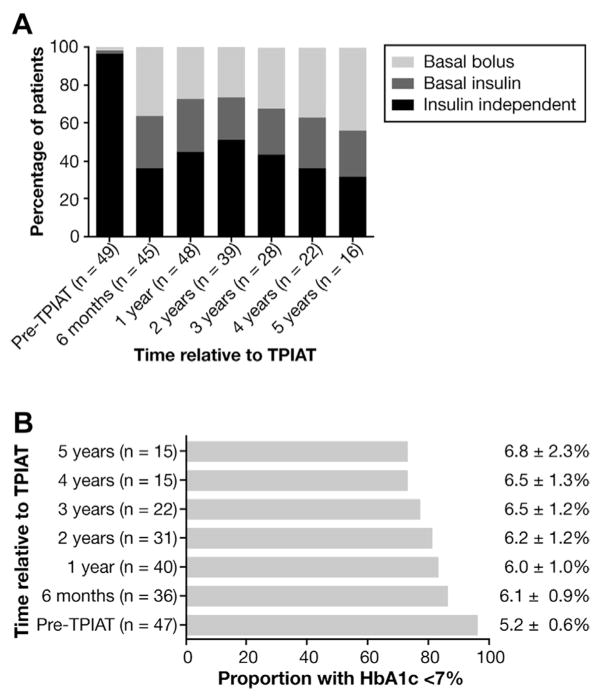
Results: All 49 patients studied required narcotics before TPIAT (45 daily users and 4 intermittent users); 2 had insulin-treated diabetes. At 1 year after TPIAT, 22 out of 48 patients (46%) reported no use of narcotic pain medications (P < .001 vs baseline). Health-related quality of life score, measured by the physical and mental component summary score, increased by approximately 1 standard deviation from the population mean (P < .001 for the physical component summary; P = .019 for the mental component summary). At 1 year after TPIAT, 21 out of 48 patients (45%) were insulin independent; their mean percent glycosylated hemoglobin A1c at 1 year after TPIAT was 6.0% ± 0.9% (5.2% ± 0.6% pre-TPIAT).
Conclusions: Patients with recurrent acute pancreatitis but lacking clear chronic pancreatitis benefit from TPIAT, with outcomes similar to those previously described for patients with chronic pancreatitis (improved quality of life and reduced narcotic use). For these patients who have otherwise limited surgical treatment options, TPIAT can be considered when medical and endoscopic therapies have failed.
Keywords: CP; HRQL; clinical trial; pancreas.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflicts.
Figures



Comment in
-
Total Pancreatectomy With Islet Autotransplantation Improves Quality of Life in Patients With Refractory Recurrent Acute Pancreatitis.Clin Gastroenterol Hepatol. 2017 Feb;15(2):321. doi: 10.1016/j.cgh.2016.09.005. Epub 2016 Sep 14. Clin Gastroenterol Hepatol. 2017. PMID: 27639332 No abstract available.
-
Reply.Clin Gastroenterol Hepatol. 2017 Feb;15(2):321-322. doi: 10.1016/j.cgh.2016.10.016. Epub 2016 Oct 21. Clin Gastroenterol Hepatol. 2017. PMID: 27777065 No abstract available.
References
-
- Guda NM, Romagnuolo J, Freeman ML. Recurrent and relapsing pancreatitis. Curr Gastroenterol Rep. 2011;13:140–149. - PubMed
-
- Romagnuolo J, Guda N, Freeman M, et al. Preferred designs, outcomes, and analysis strategies for treatment trials in idiopathic recurrent acute pancreatitis. Gastrointest Endosc. 2008;68:966–974. - PubMed
-
- Roberts JR, Romagnuolo J. Endoscopic therapy for acute recurrent pancreatitis. Gastrointest Endosc Clin North Am. 2013;23:803–819. - PubMed
-
- Bertin C, Pelletier AL, Vullierme MP, et al. Pancreas divisum is not a cause of pancreatitis by itself but acts as a partner of genetic mutations. Am J Gastroenterol. 2012;107:311–317. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
