

A Standardized Discharge Process Decreases Length of Stay for Ventilator-Dependent Children
- PMID: 26966133
- PMCID: PMC4811306
- DOI: 10.1542/peds.2015-0637
A Standardized Discharge Process Decreases Length of Stay for Ventilator-Dependent Children
Abstract
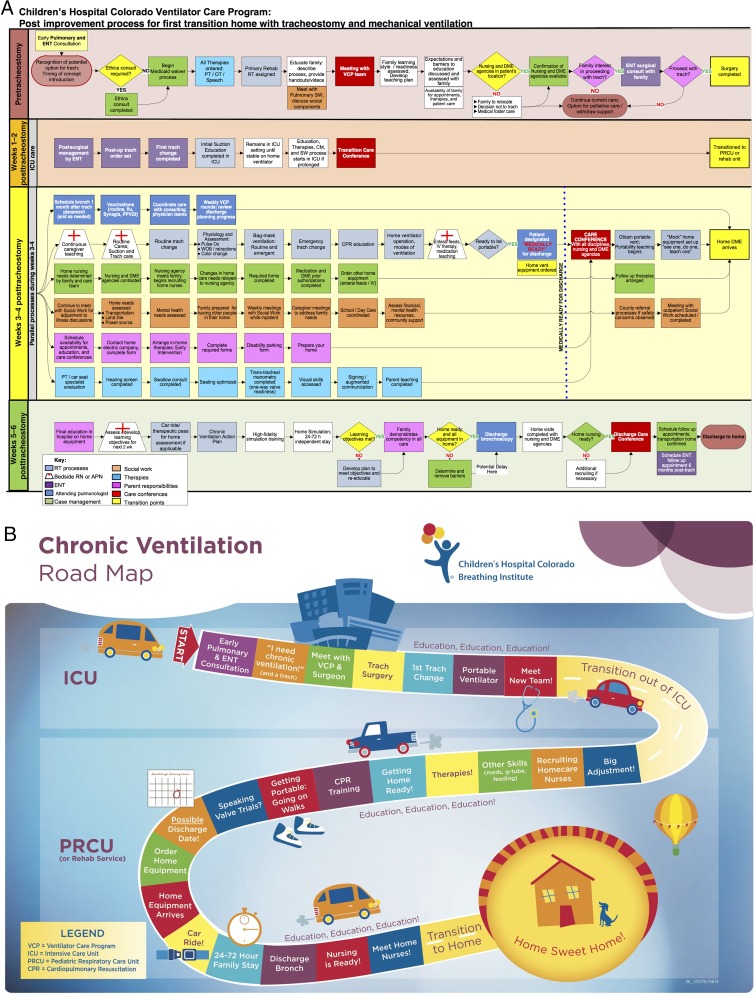
Objective: Children who require chronic mechanical ventilation via tracheostomy are medically complex and require prolonged hospitalization, placing a heavy burden on caregivers and hospital systems. We developed an interdisciplinary Ventilator Care Program to relieve this burden, through improved communication and standardized care. We hypothesized that a standardized team approach to the discharge of tracheostomy- and ventilator-dependent children would decrease length of stay (LOS), reduce patient costs, and improve safety.
Methods: We used process mapping to standardize the discharge process for children requiring chronic ventilation. Interventions included developing education materials, a Chronic Ventilation Road Map for caregivers, utilization of the electronic medical record to track discharge readiness, team-based care coordination, and timely case management to arrange home nursing. We aimed to decrease overall and pediatric respiratory care unit LOS as the primary outcomes. We also analyzed secondary outcomes (mortality, emergency department visits, unplanned readmissions), and per-patient hospital costs during 2-year "preintervention" and "postintervention" periods (n = 18 and 30, respectively).
Results: Patient demographics were not different between groups. As compared with the preintervention cohort, the overall LOS decreased 42% (P = .002). Pediatric respiratory care unit LOS decreased 56% (P = .001). As a result, unplanned readmissions, emergency department visits, and mortality were not increased. Direct costs per hospitalization were decreased by an average of 43% (P = .01).
Conclusions: Although LOS remained high, a standardized discharge process for chronically ventilated children by an interdisciplinary Ventilator Care Program team resulted in decreased LOS and costs without a negative impact on patient safety.
Copyright © 2016 by the American Academy of Pediatrics.
Conflict of interest statement
Figures

References
-
- Bach JR, Intintola P, Alba AS, Holland IE. The ventilator-assisted individual. Cost analysis of institutionalization vs rehabilitation and in-home management. Chest. 1992;101(1):26–30 - PubMed
-
- King AC. Long-term home mechanical ventilation in the United States. Respir Care. 2012;57(6):921–930; discussion 930–922 - PubMed
-
- Benneyworth BD, Gebremariam A, Clark SJ, Shanley TP, Davis MM. Inpatient health care utilization for children dependent on long-term mechanical ventilation. Pediatrics. 2011;127(6). Available at: www.pediatrics.org/cgi/content/full/127/6/e1533 - PMC - PubMed
-
- Cohen E, Berry JG, Camacho X, Anderson G, Wodchis W, Guttmann A. Patterns and costs of health care use of children with medical complexity. Pediatrics. 2012;130(6). Available at: www.pediatrics.org/cgi/content/full/130/6/e1463 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
