

Implementation and Operational Research: What Happens After a Negative Test for Tuberculosis? Evaluating Adherence to TB Diagnostic Algorithms in South African Primary Health Clinics
- PMID: 26966843
- PMCID: PMC4804742
- DOI: 10.1097/QAI.0000000000000907
Implementation and Operational Research: What Happens After a Negative Test for Tuberculosis? Evaluating Adherence to TB Diagnostic Algorithms in South African Primary Health Clinics
Abstract
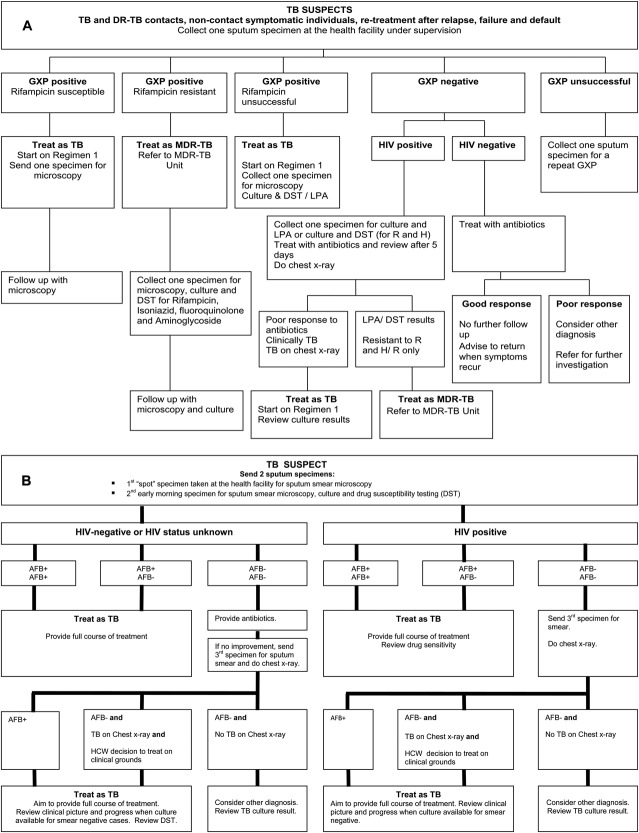
Introduction and background: Diagnostic tests for tuberculosis (TB) using sputum have suboptimal sensitivity among HIV-positive persons. We assessed health care worker adherence to TB diagnostic algorithms after negative sputum test results.
Methods: The XTEND (Xpert for TB-Evaluating a New Diagnostic) trial compared outcomes among people tested for TB in primary care clinics using Xpert MTB/RIF vs. smear microscopy as the initial test. We analyzed data from XTEND participants who were HIV positive or HIV status unknown, whose initial sputum Xpert MTB/RIF or microscopy result was negative. If chest radiography, sputum culture, or hospital referral took place, the algorithm for TB diagnosis was considered followed. Analysis of intervention (Xpert MTB/RIF) effect on algorithm adherence used methods for cluster-randomized trials with small number of clusters.
Results: Among 4037 XTEND participants with initial negative test results, 2155 (53%) reported being or testing HIV positive and 540 (14%) had unknown HIV status. Among 2155 HIV-positive participants [684 (32%) male, mean age 37 years (range, 18-79 years)], there was evidence of algorithm adherence among 515 (24%). Adherence was less likely among persons tested initially with Xpert MTB/RIF vs. smear [14% (142/1031) vs. 32% (364/1122), adjusted risk ratio 0.34 (95% CI: 0.17 to 0.65)] and for participants with unknown vs. positive HIV status [59/540 (11%) vs. 507/2155 (24%)].
Conclusions: We observed poorer adherence to TB diagnostic algorithms among HIV-positive persons tested initially with Xpert MTB/RIF vs. microscopy. Poor adherence to TB diagnostic algorithms and incomplete coverage of HIV testing represents a missed opportunity to diagnose TB and HIV, and may contribute to TB mortality.
Conflict of interest statement
The authors have no funding or conflicts of interest to disclose
Figures
References
-
- WHO. Global TB Report. Geneva, Switzerland; 2014. Available at: http://www.who.int/tb/publications/global_report/en/. WHO/HTM/TB/2014.08. Accessed March 12, 2015.
-
- Bradshaw D, Pillay-Van Wyk V, Laubscher R, et al. Cause of Death Statistics for South Africa: Challenges and Possibilities for Improvement. Cape Town, South Africa: Burden of Disease Research Unit, Medical Research Council; 2010. Available at: www.mrc.ac.za/bod/cause_death_statsSA.pdf. Accessed March 12, 2015.
-
- Mortality and causes of death in South Africa, 2013. Findings from Death Notification. Pretoria: Statistics South Africa; 2014. Available at: http://beta2.statssa.gov.za/publications/P03093/P030932013.pdf. Accessed March 12, 2015.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
