

HIV Incidence Among Men Who Have Sex With Men After Diagnosis With Sexually Transmitted Infections
- PMID: 26967302
- PMCID: PMC4789769
- DOI: 10.1097/OLQ.0000000000000423
HIV Incidence Among Men Who Have Sex With Men After Diagnosis With Sexually Transmitted Infections
Abstract
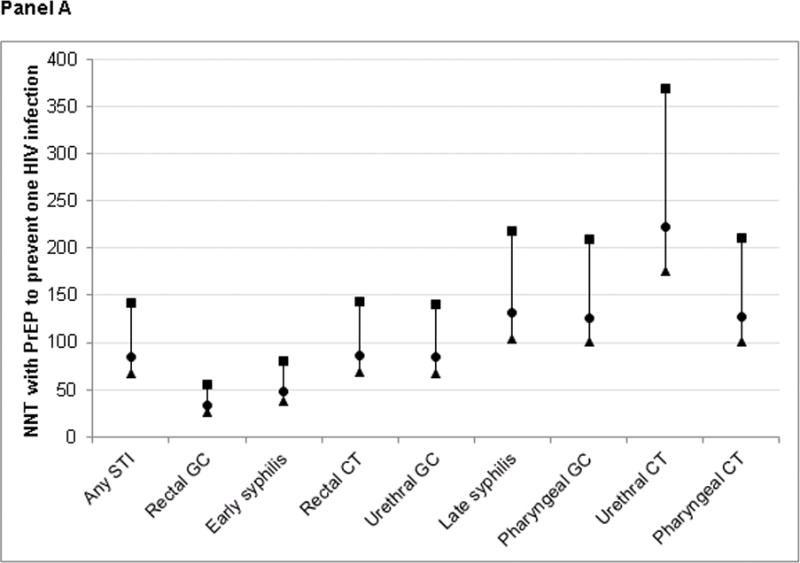
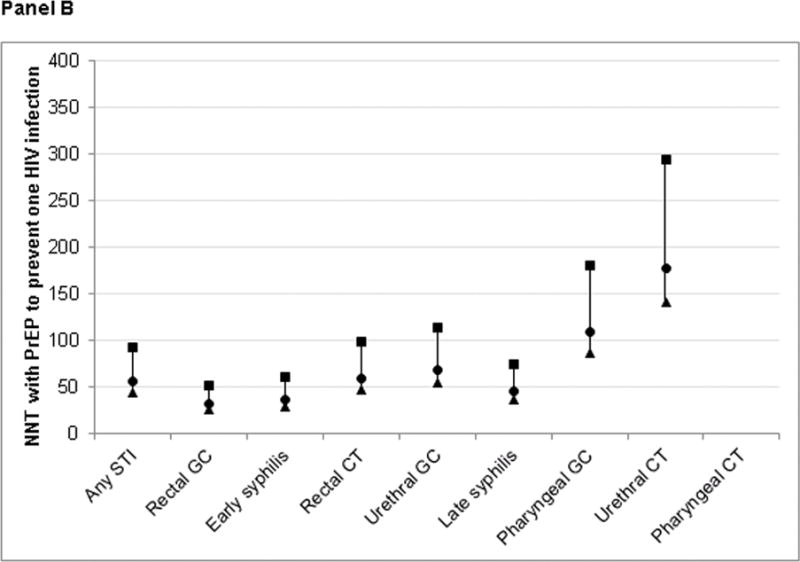
Background: Men who have sex with men (MSM) are at high risk for acquiring HIV infection after diagnosis with other sexually transmitted infections (STIs). Identifying the STIs associated with the greatest risk of subsequent HIV infection could help target prevention interventions, particularly preexposure prophylaxis (PrEP).
Methods: Using matched HIV and STI surveillance data from Washington State from January 1, 2007, to June 30, 2013, we calculated the incidence of new HIV diagnoses after different STI diagnoses among MSM. Men entered observation at the time of their first STI diagnosis during the study period and exited at HIV diagnosis or June 30, 2013. Cox proportional hazards regression was used to conduct a global comparison of rates.
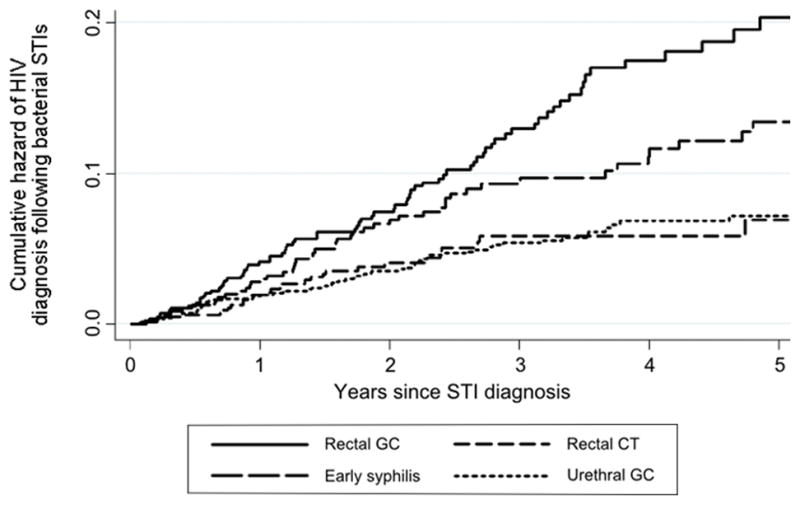
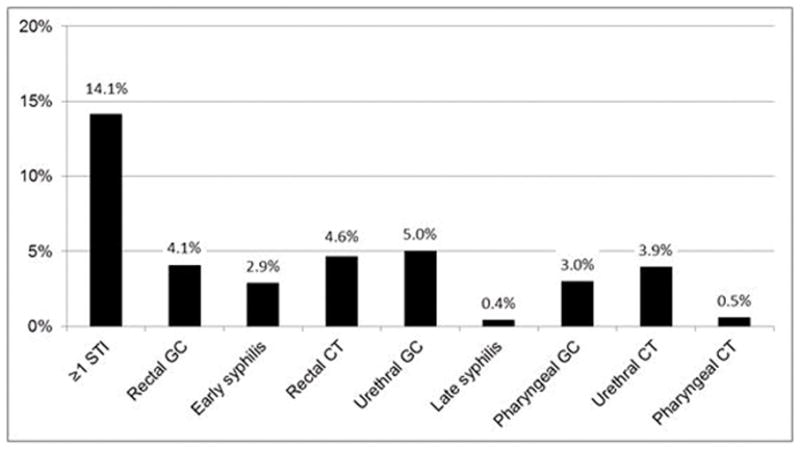
Results: From January 1, 2007, to June 30, 2013, 6577 HIV-negative MSM were diagnosed as having 10,080 bacterial STIs at 8371 unique time points and followed for 17,419 person-years. Two hundred eighty (4.3%) men were subsequently diagnosed as having HIV infection for an overall incidence of 1.6 per 100 person-years (95% confidence interval, 1.4-1.8). The estimated incidence of HIV diagnoses among all MSM in the state was 0.4 per 100 person-years. Men who have sex with men were at the greatest risk for HIV diagnosis after being diagnosed as having rectal gonorrhea (HIV incidence, 4.1 per 100 person-years), followed by early syphilis (2.8), urethral gonorrhea (1.6), rectal chlamydial infection (1.6), pharyngeal gonorrhea (1.1), late syphilis (1.0), and urethral chlamydial infection (0.6; P < 0.0001 overall).
Conclusions: Men who have sex with men diagnosed as having rectal gonorrhea and early syphilis were at the greatest risk for being diagnosed as having HIV infection after STI diagnosis. These men should be prioritized for more intensive prevention interventions, including PrEP.
Conflict of interest statement
Dr. Golden has received research support from Cempra Pharmaceuticals and Melina Pharmaceuticals. The remaining authors have no potential conflicts of interest to declare.
Figures
References
-
- Cohen CR, Plummer FA, Mugo N, et al. Increased interleukin-10 in the the endocervical secretions of women with non-ulcerative sexually transmitted diseases: a mechanism for enhanced HIV-1 transmission? AIDS. 1999;13(3):327–32. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
