

[Fever in children returning from travel]
- PMID: 26968306
- PMCID: PMC7127267
- DOI: 10.1016/j.arcped.2015.12.021
[Fever in children returning from travel]
Abstract
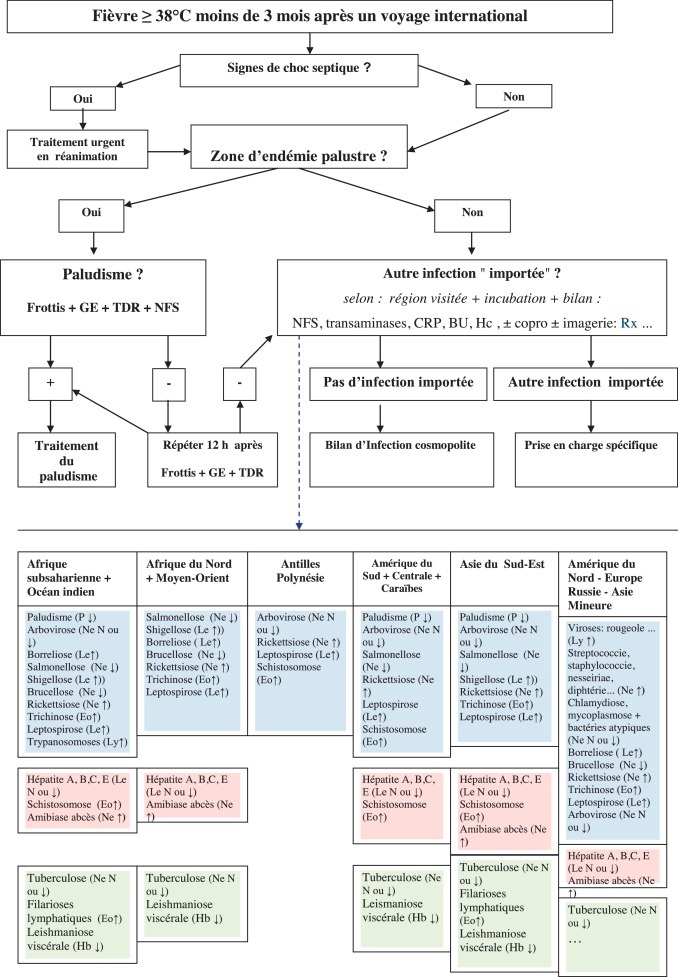
Child travelers are numerous, exposed to the risk of diseases, both infectious and noninfectious, for which practitioners often lack experience. The assessment of febrile returning child travelers is becoming more frequent and challenging. The question of previous travel should be foremost in the checklist of the interview of any febrile child traveler, because this implies a possible tropical disease such as malaria that may be life-threatening. These need to be investigated and treated effectively and rapidly. There are highly contagious infections that could pose public health risks requiring implementation of hygienic and public health measures. A detailed immunization, medical, and travel history for exposure to infectious risks using geographic, seasonal, environmental, sociocultural, and epidemiological data are needed. Along with clinical examination and elementary first-line investigations, the history should guide second-line exams, which will provide the etiology and optimal treatment in approximately 75 % of cases. The majority of children will have a cosmopolitan infection that resolves spontaneously or is simple to treat. Malaria will need urgent and specific treatment. This article describes guidance on first-line evaluation and management of febrile child travelers as recommended in France.
Les enfants voyageurs sont des millions dans le monde et sont exposés à de nombreux risques, infectieux ou non, dont les praticiens n’ont pas toujours l’expérience. La consultation d’un enfant fébrile après un voyage est de plus en plus fréquente. Ainsi, la notion d’antécédent de voyage doit être recherchée devant tout enfant fébrile. La démarche diagnostique prend en compte prioritairement des pathologies intertropicales potentiellement graves, comme le paludisme, qui exigent d’être recherchées et traitées efficacement sans délai. Rapidement sont recherchées des infections contagieuses à risque épidémique qui nécessitent la mise en place de mesures d’hygiène et de santé publique. L’interrogatoire évalue les caractéristiques de la fièvre, les vaccinations réalisées, les antécédents médico-chirurgicaux et les risques d’exposition aux infections lors du voyage d’après les données géographiques, saisonnières, environnementales, socioculturelles et épidémiologiques. Il oriente avec les données cliniques et paracliniques élémentaires certains examens complémentaires qui permettent un diagnostic étiologique et un traitement optimal dans près de 75 % des cas. La majorité des causes de fièvre des enfants au retour de voyage sont des infections cosmopolites. En cas de paludisme, le traitement antipaludique est une urgence. Cet article décrit la démarche diagnostique et la prise en charge recommandée en France devant un enfant fébrile de retour de voyage.
Copyright © 2016 Elsevier Masson SAS. All rights reserved.
Figures
 : < 14 j ;
: < 14 j ;  : 2–6 sem ;
: 2–6 sem ;  : > 6 sem.
: > 6 sem.Similar articles
-
Fever in the Returning Traveler.Dtsch Arztebl Int. 2022 Jun 7;119(22):400-407. doi: 10.3238/arztebl.m2022.0182. Dtsch Arztebl Int. 2022. PMID: 35469592 Free PMC article. Review.
-
Fever in the Returning Traveler.Infect Dis Clin North Am. 2018 Mar;32(1):163-188. doi: 10.1016/j.idc.2017.10.009. Infect Dis Clin North Am. 2018. PMID: 29406974 Free PMC article. Review.
-
Fever in the returning child traveller: approach to diagnosis and management.Arch Dis Child. 2014 Oct;99(10):938-43. doi: 10.1136/archdischild-2012-303196. Epub 2014 Mar 25. Arch Dis Child. 2014. PMID: 24667950
-
Development and Implementation of the Ebola Traveler Monitoring Program and Clinical Outcomes of Monitored Travelers during October - May 2015, Minnesota.PLoS One. 2016 Dec 1;11(12):e0166797. doi: 10.1371/journal.pone.0166797. eCollection 2016. PLoS One. 2016. PMID: 27907013 Free PMC article.
-
[Fever in returned travelers].Harefuah. 2010 Sep;149(9):598-603, 618. Harefuah. 2010. PMID: 21302477 Hebrew.
Cited by
-
Conduite à tenir devant un enfant fébrile au retour de voyage.J Pediatr Pueric. 2020 Jun;33(3):118-145. doi: 10.1016/j.jpp.2020.04.002. Epub 2020 Apr 27. J Pediatr Pueric. 2020. PMID: 32341631 Free PMC article. French.
-
Conducta práctica ante un niño febril al regresar de un viaje.EMC Pediatr. 2019 Aug;54(3):1-22. doi: 10.1016/S1245-1789(19)42593-6. Epub 2019 Aug 26. EMC Pediatr. 2019. PMID: 32308527 Free PMC article. Review. Spanish.
References
-
- Newman-Klee C., D’Acremont V., Newman C.J. Incidence and type of illness when travelling to the tropics. A prospective controlled study of children and their parents. Am J Trop Med Hyg. 2007;77:764–769. - PubMed
-
- Hagman S., Neugebauer R., Eli Schwartz E. Illness in children after international travel: analysis from the geosentinelle Surveillance Network. Pediatrics. 2010;125:e1072–e1080. - PubMed
-
- Naudin J., Blondé R., Alberti C. Aetiology and epidemiology of fever in children presenting to the emergency departement of a french paediatric tertiary care center after international travel. Arch Dis Child. 2012;97:107–111. - PubMed
-
- Bottieau E., Clerinx J., Van den Enden E. Fever after a stay in the tropics: diagnostic predictors of the leading tropical conditions. Medicine (Baltimore) 2007;86:18–25. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
