

The association between lactate, mean arterial pressure, central venous oxygen saturation and peripheral temperature and mortality in severe sepsis: a retrospective cohort analysis
- PMID: 26968689
- PMCID: PMC4788911
- DOI: 10.1186/s13054-016-1243-3
The association between lactate, mean arterial pressure, central venous oxygen saturation and peripheral temperature and mortality in severe sepsis: a retrospective cohort analysis
Abstract
Background: During resuscitation in severe sepsis and septic shock, several goals are set. However, usually not all goals are equally met. The aim of this study is to determine the relative importance of the different goals, such as mean arterial pressure (MAP), lactate, central venous oxygen saturation (ScvO2) and central to forefoot temperature (delta-T), and how they relate to intensive care unit (ICU) and hospital mortality.
Methods: In a retrospective cohort study in a 20-bed mixed medical and surgical ICU of a teaching hospital we studied consecutive critically ill patients who were admitted for confirmed infection and severe sepsis or septic shock between 2008 and 2014. All validated MAP, lactate levels, ScvO2 and delta-T for the first 24 hours of ICU treatment were extracted from a clinical database. Logistic regression analyses were performed on validated measurements in the first hour after admission and on mean values over 24 hours. Patients were categorized by MAP (24-hour mean below or above 65 mmHg) and lactate (24-hour mean below or above 2 mmol/l) for Cox regression analysis.
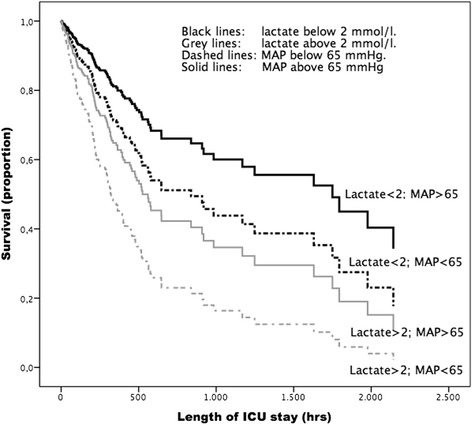
Results: From 837 patients, 821 were eligible for analysis. All had MAP and lactate measurements. The delta-T was available in 812 (99%) and ScvO2 was available for 193 out of these patients (23.5%). Admission lactate (p < 0.001) and admission MAP (p < 0.001) were independent predictors of ICU and hospital mortality. The 24-hour mean values for lactate, MAP and delta-T were all independent predictors of ICU mortality. Hospital mortality was independently predicted by the 24-hour mean lactate (odds ratio (OR) 1.34, 95% confidence interval (CI) 1.30-1.40, p = 0.001) mean MAP (OR 0.96, 95% CI 0.95-0.97, p = 0.001) and mean delta-T (OR 1.09, 95% CI 1.06-1.12, p = 0.001). Patients with a 24-hour mean lactate below 2 mmol/l and a 24-hour mean MAP above 65 mmHg had the best survival, followed by patients with a low lactate and a low MAP.
Conclusions: Admission MAP and lactate independently predicted ICU and hospital mortality. The 24-hour mean lactate, mean MAP and mean delta-T independently predicted hospital mortality. A Cox regression analysis showed that 24-hour mean lactate above 2 mmol/l is the strongest predictor for ICU mortality.
Keywords: Central venous oxygen saturation; ICU; Lactate; Mean arterial pressure; Outcome; Peripheral temperature; Resuscitation; Sepsis.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
