

Web-Based Interventions Targeting Cardiovascular Risk Factors in Middle-Aged and Older People: A Systematic Review and Meta-Analysis
- PMID: 26968879
- PMCID: PMC4808240
- DOI: 10.2196/jmir.5218
Web-Based Interventions Targeting Cardiovascular Risk Factors in Middle-Aged and Older People: A Systematic Review and Meta-Analysis
Abstract
Background: Web-based interventions can improve single cardiovascular risk factors in adult populations. In view of global aging and the associated increasing burden of cardiovascular disease, older people form an important target population as well.
Objective: In this systematic review and meta-analysis, we evaluated whether Web-based interventions for cardiovascular risk factor management reduce the risk of cardiovascular disease in older people.
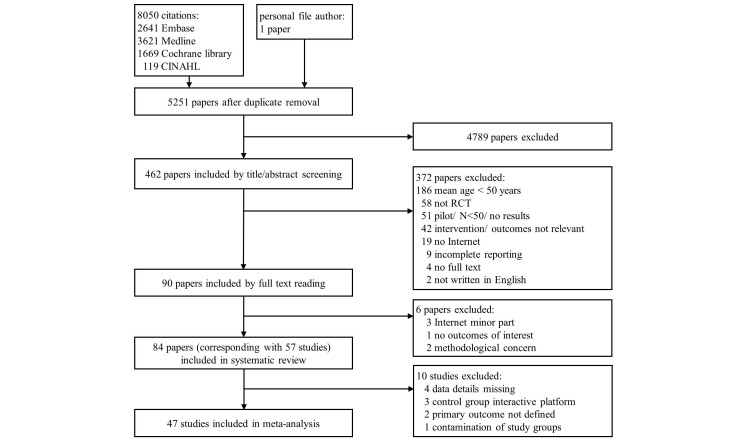
Methods: Embase, Medline, Cochrane and CINAHL were systematically searched from January 1995 to November 2014. Search terms included cardiovascular risk factors and diseases (specified), Web-based interventions (and synonyms) and randomized controlled trial. Two authors independently performed study selection, data-extraction and risk of bias assessment. In a meta-analysis, outcomes regarding treatment effects on cardiovascular risk factors (blood pressure, glycated hemoglobin A1c (HbA1C), low-density lipoprotein (LDL) cholesterol, smoking status, weight and physical inactivity) and incident cardiovascular disease were pooled with random effects models.
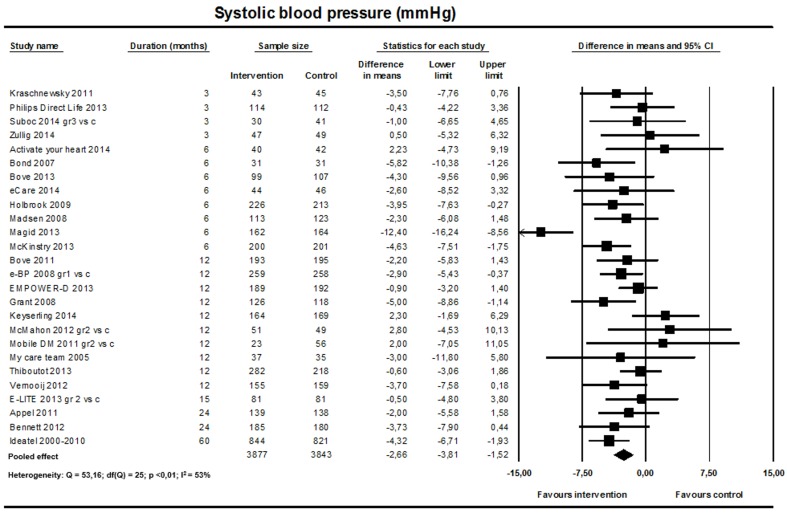
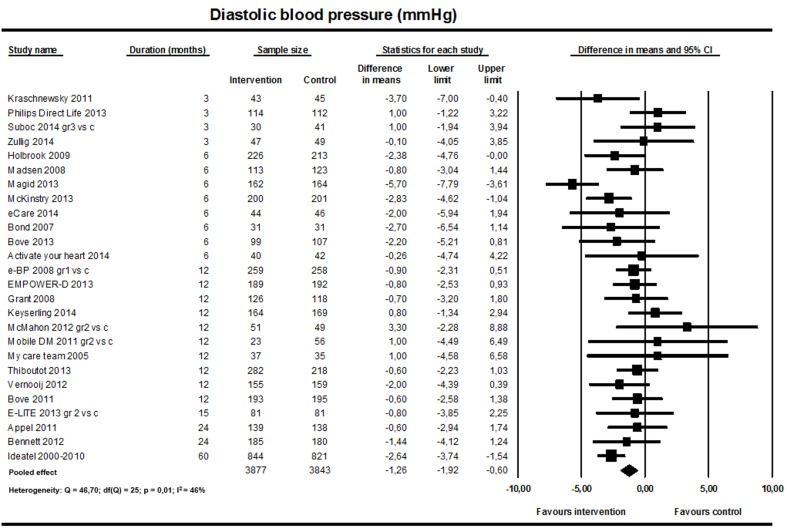
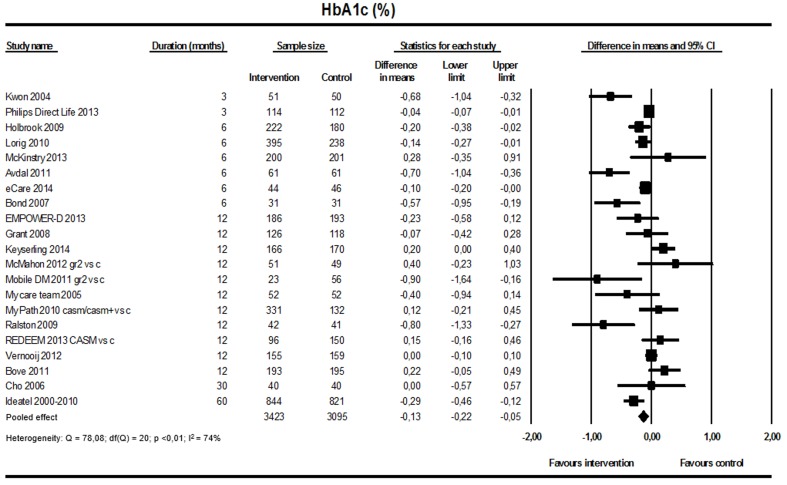
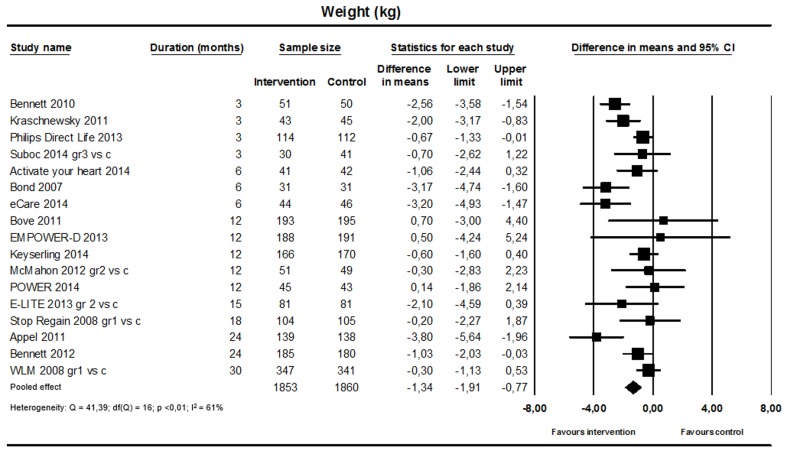
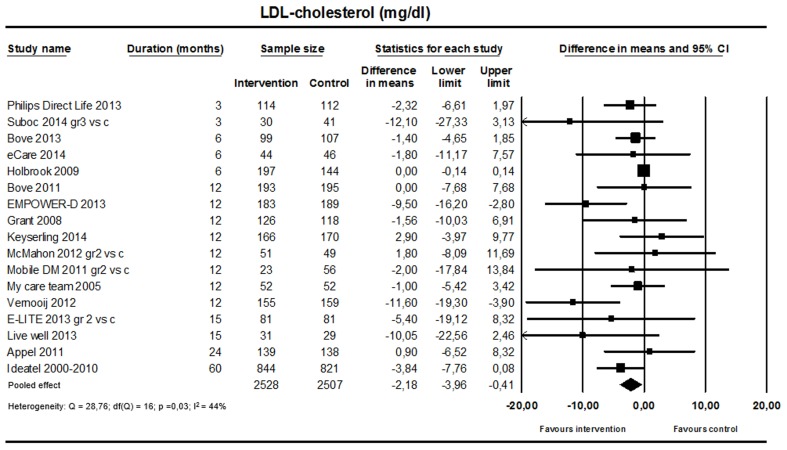
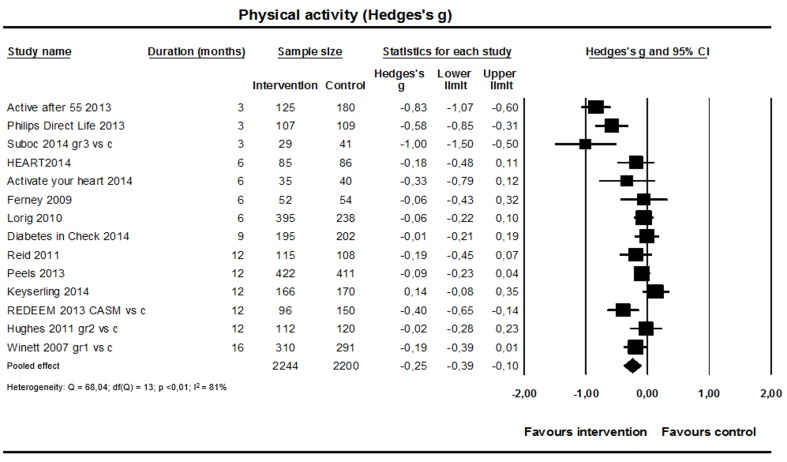
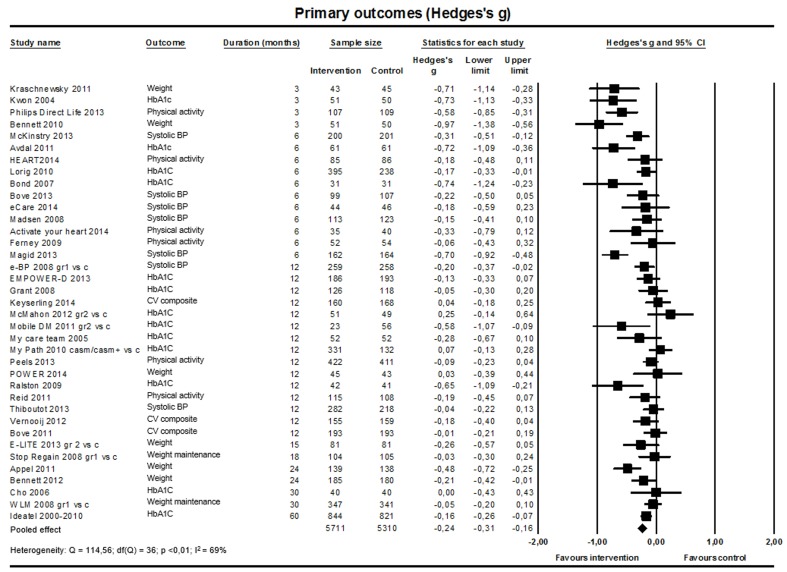
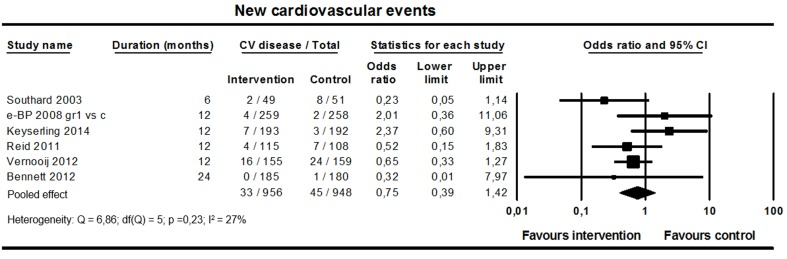
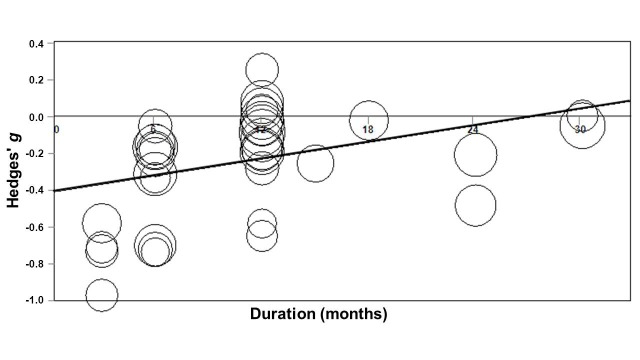
Results: A total of 57 studies (N=19,862) fulfilled eligibility criteria and 47 studies contributed to the meta-analysis. A significant reduction in systolic blood pressure (mean difference -2.66 mmHg, 95% CI -3.81 to -1.52), diastolic blood pressure (mean difference -1.26 mmHg, 95% CI -1.92 to -0.60), HbA1c level (mean difference -0.13%, 95% CI -0.22 to -0.05), LDL cholesterol level (mean difference -2.18 mg/dL, 95% CI -3.96 to -0.41), weight (mean difference -1.34 kg, 95% CI -1.91 to -0.77), and an increase of physical activity (standardized mean difference 0.25, 95% CI 0.10-0.39) in the Web-based intervention group was found. The observed effects were more pronounced in studies with short (<12 months) follow-up and studies that combined the Internet application with human support (blended care). No difference in incident cardiovascular disease was found between groups (6 studies).
Conclusions: Web-based interventions have the potential to improve the cardiovascular risk profile of older people, but the effects are modest and decline with time. Currently, there is insufficient evidence for an effect on incident cardiovascular disease. A focus on long-term effects, clinical endpoints, and strategies to increase sustainability of treatment effects is recommended for future studies.
Keywords: aging; cardiovascular disease; eHealth; meta-analysis; older people; prevention; systematic review.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- World Health Organization. National Institute on Aging. National Institutes of Health . Global Health and Aging. Geneva: World Health Organization; 2011. [2016-02-22]. http://www.who.int/ageing/publications/global_health.pdf .
-
- Chow CK, Jolly S, Rao-Melacini P, Fox KA, Anand SS, Yusuf S. Association of diet, exercise, and smoking modification with risk of early cardiovascular events after acute coronary syndromes. Circulation. 2010 Feb 16;121(6):750–758. doi: 10.1161/CIRCULATIONAHA.109.891523. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=20124123 CIRCULATIONAHA.109.891523 - DOI - PubMed
-
- Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ. 2009;338:b1665. http://www.bmj.com/cgi/pmidlookup?view=long&pmid=19454737 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
