

Adjuvant sunitinib or sorafenib for high-risk, non-metastatic renal-cell carcinoma (ECOG-ACRIN E2805): a double-blind, placebo-controlled, randomised, phase 3 trial
- PMID: 26969090
- PMCID: PMC4878938
- DOI: 10.1016/S0140-6736(16)00559-6
Adjuvant sunitinib or sorafenib for high-risk, non-metastatic renal-cell carcinoma (ECOG-ACRIN E2805): a double-blind, placebo-controlled, randomised, phase 3 trial
Erratum in
-
Department of Error.Lancet. 2016 May 14;387(10032):1998. doi: 10.1016/S0140-6736(16)30470-6. Lancet. 2016. PMID: 27203774 No abstract available.
Abstract
Background: Renal-cell carcinoma is highly vascular, and proliferates primarily through dysregulation of the vascular endothelial growth factor (VEGF) pathway. We tested sunitinib and sorafenib, two oral anti-angiogenic agents that are effective in advanced renal-cell carcinoma, in patients with resected local disease at high risk for recurrence.
Methods: In this double-blind, placebo-controlled, randomised, phase 3 trial, we enrolled patients at 226 study centres in the USA and Canada. Eligible patients had pathological stage high-grade T1b or greater with completely resected non-metastatic renal-cell carcinoma and adequate cardiac, renal, and hepatic function. Patients were stratified by recurrence risk, histology, Eastern Cooperative Oncology Group (ECOG) performance status, and surgical approach, and computerised double-blind randomisation was done centrally with permuted blocks. Patients were randomly assigned (1:1:1) to receive 54 weeks of sunitinib 50 mg per day orally throughout the first 4 weeks of each 6 week cycle, sorafenib 400 mg twice per day orally throughout each cycle, or placebo. Placebo could be sunitinib placebo given continuously for 4 weeks of every 6 week cycle or sorafenib placebo given twice per day throughout the study. The primary objective was to compare disease-free survival between each experimental group and placebo in the intention-to-treat population. All treated patients with at least one follow-up assessment were included in the safety analysis. This trial is registered with ClinicalTrials.gov, number NCT00326898.
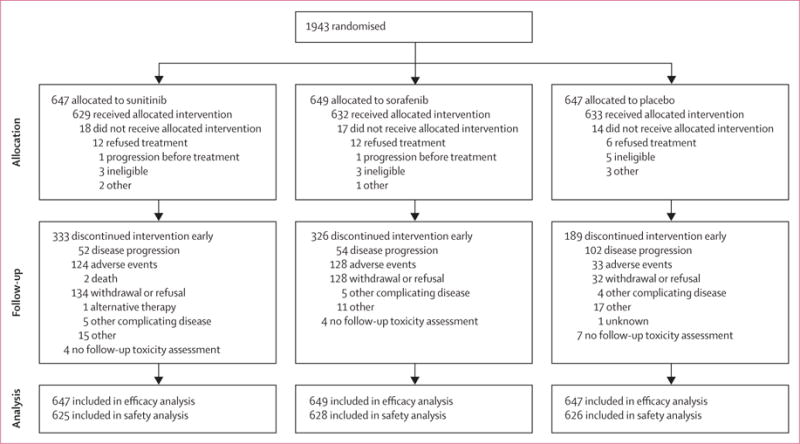
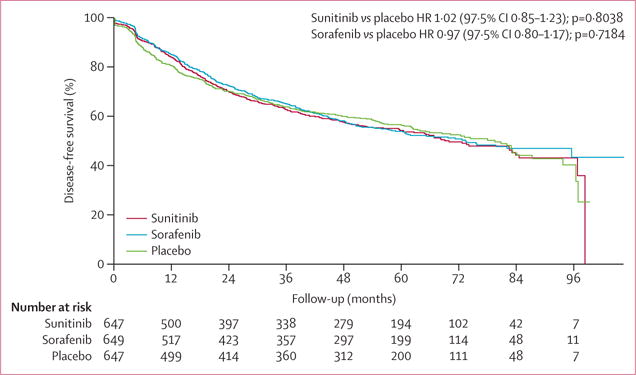
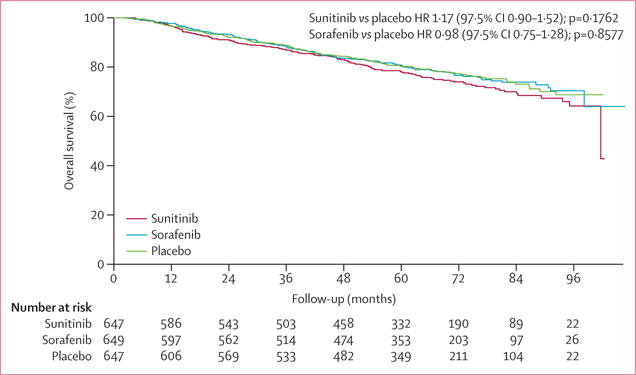
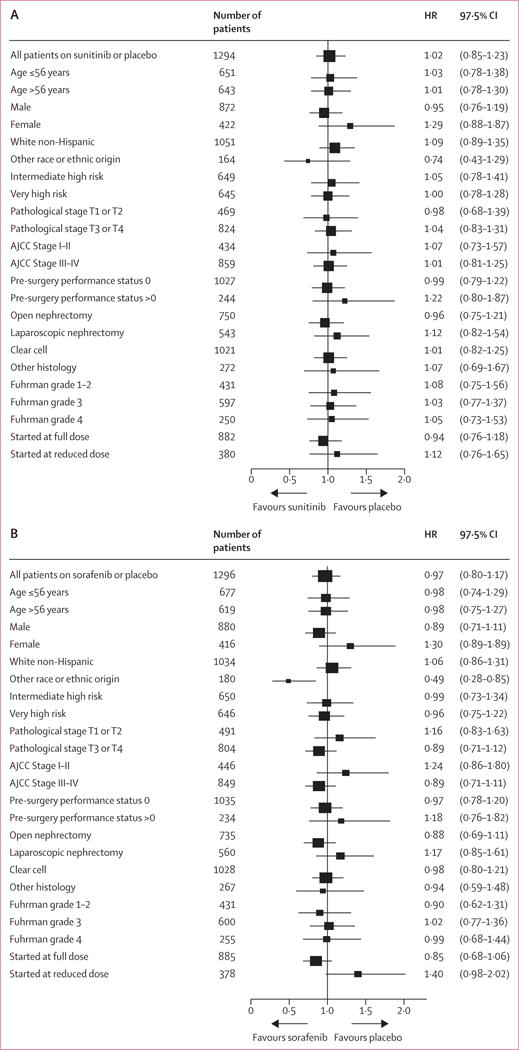
Findings: Between April 24, 2006, and Sept 1, 2010, 1943 patients from the National Clinical Trials Network were randomly assigned to sunitinib (n=647), sorafenib (n=649), or placebo (n=647). Following high rates of toxicity-related discontinuation after 1323 patients had enrolled (treatment discontinued by 193 [44%] of 438 patients on sunitinib, 199 [45%] of 441 patients on sorafenib), the starting dose of each drug was reduced and then individually titrated up to the original full doses. On Oct 16, 2014, because of low conditional power for the primary endpoint, the ECOG-ACRIN Data Safety Monitoring Committee recommended that blinded follow-up cease and the results be released. The primary analysis showed no significant differences in disease-free survival. Median disease-free survival was 5·8 years (IQR 1·6-8·2) for sunitinib (hazard ratio [HR] 1·02, 97·5% CI 0·85-1·23, p=0·8038), 6·1 years (IQR 1·7-not estimable [NE]) for sorafenib (HR 0·97, 97·5% CI 0·80-1·17, p=0·7184), and 6·6 years (IQR 1·5-NE) for placebo. The most common grade 3 or worse adverse events were hypertension (105 [17%] patients on sunitinib and 102 [16%] patients on sorafenib), hand-foot syndrome (94 [15%] patients on sunitinib and 208 [33%] patients on sorafenib), rash (15 [2%] patients on sunitinib and 95 [15%] patients on sorafenib), and fatigue 110 [18%] patients on sunitinib [corrected]. There were five deaths related to treatment or occurring within 30 days of the end of treatment; one patient receiving sorafenib died from infectious colitis while on treatment and four patients receiving sunitinib died, with one death due to each of neurological sequelae, sequelae of gastric perforation, pulmonary embolus, and disease progression. Revised dosing still resulted in high toxicity.
Interpretation: Adjuvant treatment with the VEGF receptor tyrosine kinase inhibitors sorafenib or sunitinib showed no survival benefit relative to placebo in a definitive phase 3 study. Furthermore, substantial treatment discontinuation occurred because of excessive toxicity, despite dose reductions. These results provide a strong rationale against the use of these drugs for high-risk kidney cancer in the adjuvant setting and suggest that the biology of cancer recurrence might be independent of angiogenesis.
Funding: US National Cancer Institute and ECOG-ACRIN Cancer Research Group, Pfizer, and Bayer.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
JPD reports personal fees for Pfizer consultation. All other authors declare no competing interests.
Figures
Comment in
-
Adjuvant therapy for renal-cell carcinoma: settled for now.Lancet. 2016 May 14;387(10032):1973-4. doi: 10.1016/S0140-6736(16)00653-X. Epub 2016 Mar 9. Lancet. 2016. PMID: 26969091 No abstract available.
-
Kidney cancer: No advantage of adjuvant sunitinib or sorafenib.Nat Rev Urol. 2016 May;13(5):240-1. doi: 10.1038/nrurol.2016.63. Epub 2016 Mar 31. Nat Rev Urol. 2016. PMID: 27030525 No abstract available.
-
Kidney cancer: Rest ASSUREd, much can be learned from adjuvant studies in renal cancer.Nat Rev Nephrol. 2016 Jun;12(6):317-8. doi: 10.1038/nrneph.2016.58. Epub 2016 Apr 25. Nat Rev Nephrol. 2016. PMID: 27108841 Free PMC article.
-
ASSURE vs. S-TRAC: conflicting results of adjuvant treatments for kidney cancer in the era of targeted agents and genomics.Ann Transl Med. 2016 Oct;4(Suppl 1):S14. doi: 10.21037/atm.2016.10.45. Ann Transl Med. 2016. PMID: 27867982 Free PMC article. No abstract available.
-
Re: Adjuvant Sunitinib in High-risk Renal-cell Carcinoma After Nephrectomy.Eur Urol. 2018 Jul;74(1):119-121. doi: 10.1016/j.eururo.2018.01.036. Epub 2018 Feb 9. Eur Urol. 2018. PMID: 29433972 No abstract available.
References
-
- International Agency for Research on Cancer. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. http://globocan.iarc.fr/Pages/fact_sheets_population.aspx (accessed Dec 2, 2015)
-
- Zisman A, Pantuck AJ, Dorey F, et al. Improved prognostication of renal cell carcinoma using an integrated staging system. J Clin Oncol. 2001;19:1649–57. - PubMed
-
- Leibovich BC, Cheville JC, Lohse CM, et al. A scoring algorithm to predict survival for patients with metastatic clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. J Urol. 2005;174:1759–63. - PubMed
-
- Sorbellini M, Kattan MW, Snyder ME, et al. A postoperative prognostic nomogram predicting recurrence for patients with conventional clear cell renal cell carcinoma. J Urol. 2005;173:48–51. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- P30 CA082709/CA/NCI NIH HHS/United States
- U10 CA180847/CA/NCI NIH HHS/United States
- CA17145/CA/NCI NIH HHS/United States
- U10 CA032102/CA/NCI NIH HHS/United States
- CA180794/CA/NCI NIH HHS/United States
- CA16116/CA/NCI NIH HHS/United States
- CA21076/CA/NCI NIH HHS/United States
- U10 CA032291/CA/NCI NIH HHS/United States
- CA180847/CA/NCI NIH HHS/United States
- CA180858/CA/NCI NIH HHS/United States
- U10 CA027525/CA/NCI NIH HHS/United States
- UG1 CA233270/CA/NCI NIH HHS/United States
- CA180836/CA/NCI NIH HHS/United States
- CA180867/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- CA11789/CA/NCI NIH HHS/United States
- CA14958/CA/NCI NIH HHS/United States
- UG1 CA233329/CA/NCI NIH HHS/United States
- U10 CA013650/CA/NCI NIH HHS/United States
- CA20319/CA/NCI NIH HHS/United States
- CA32291/CA/NCI NIH HHS/United States
- N01 CA032102/CA/NCI NIH HHS/United States
- U10 CA180802/CA/NCI NIH HHS/United States
- CA41287/CA/NCI NIH HHS/United States
- U10 CA014958/CA/NCI NIH HHS/United States
- U10 CA077202/CA/NCI NIH HHS/United States
- CA80775/CA/NCI NIH HHS/United States
- CA66636/CA/NCI NIH HHS/United States
- CA077202/CA/NCI NIH HHS/United States
- U10 CA021115/CA/NCI NIH HHS/United States
- U10 CA031946/CA/NCI NIH HHS/United States
- UG1 CA189859/CA/NCI NIH HHS/United States
- CA180820/CA/NCI NIH HHS/United States
- CA27525/CA/NCI NIH HHS/United States
- CA180802/CA/NCI NIH HHS/United States
- U24 CA196172/CA/NCI NIH HHS/United States
- CA107868/CA/NCI NIH HHS/United States
- U10 CA049883/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- CA13650/CA/NCI NIH HHS/United States
- U10 CA180858/CA/NCI NIH HHS/United States
- U10 CA107868/CA/NCI NIH HHS/United States
- U10 CA017145/CA/NCI NIH HHS/United States
- CA180863/CA/NCI NIH HHS/United States
- CA189953/CA/NCI NIH HHS/United States
- U10 CA021076/CA/NCI NIH HHS/United States
- U10 CA066636/CA/NCI NIH HHS/United States
- U10 CA180836/CA/NCI NIH HHS/United States
- U10 CA080775/CA/NCI NIH HHS/United States
- P30 CA060553/CA/NCI NIH HHS/United States
- UG1 CA189828/CA/NCI NIH HHS/United States
- CA49957/CA/NCI NIH HHS/United States
- U10 CA105409/CA/NCI NIH HHS/United States
- U10 CA041287/CA/NCI NIH HHS/United States
- CA105409/CA/NCI NIH HHS/United States
- U10 CA016116/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- UG1 CA233196/CA/NCI NIH HHS/United States
- U10 CA020319/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA023318/CA/NCI NIH HHS/United States
- CA180790/CA/NCI NIH HHS/United States
- CA189859/CA/NCI NIH HHS/United States
- CA180888/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- CA15488/CA/NCI NIH HHS/United States
- U10 CA049957/CA/NCI NIH HHS/United States
- U10 CA180799/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- CA23318/CA/NCI NIH HHS/United States
- CA49883/CA/NCI NIH HHS/United States
- CA21115/CA/NCI NIH HHS/United States
- CA180821/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- UG1 CA189953/CA/NCI NIH HHS/United States
- CA180799/CA/NCI NIH HHS/United States
- P30 CA006927/CA/NCI NIH HHS/United States
- CA31946/CA/NCI NIH HHS/United States
- U10 CA015488/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
