

Increase in post-therapy tumor calcification on CT scan is not an indicator of response to therapy in low-grade serous ovarian cancer
- PMID: 26969496
- PMCID: PMC4974160
- DOI: 10.1007/s00261-016-0701-3
Increase in post-therapy tumor calcification on CT scan is not an indicator of response to therapy in low-grade serous ovarian cancer
Abstract
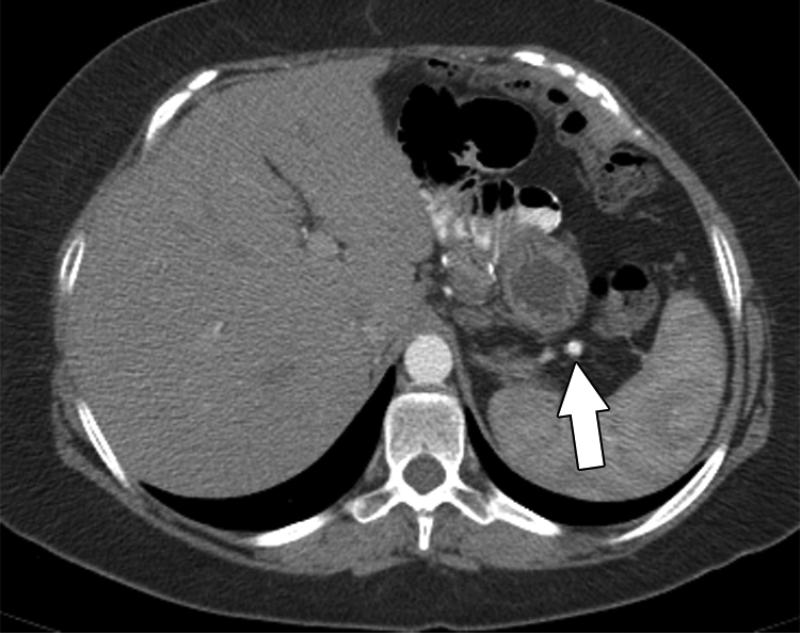
Purpose: The aim of the study was to determine if increasing post-therapy calcification in peritoneal metastases in recurrent low-grade serous ovarian carcinomas indicated response to therapy.
Materials and methods: Retrospective analysis of patients with histologically confirmed, recurrent low-grade serous ovarian carcinoma who received treatment at our institution between 2000 and 2014 was performed. Only patients who had calcified tumor implants and showed either interval increase or decrease in tumor calcification following therapy were included in the study. Pre- and post-therapy CT scans of these patients were reviewed by 2 radiologists independently. Changes in the tumor calcification status and tumor deposits size were correlated with serum CA-125 levels. Fisher's exact test was used to assess the association between peritoneal deposit and calcification status with serum CA-125 status.
Results: 35 Patients were included in the study. Based on serial serum CA 125 levels, 22 patients (63%) had progressive disease, 12 (34%) had partial response and 1 (3%) had stable disease. Using RECIST 1.1, 16 had progressive disease, 3 had partial response and 16 had stable disease. In the patients with progressive disease, post-therapy tumor calcification increased in 77% and decreased in 23%. Fischer's exact test showed that serum CA 125 change was significantly associated with change in size of peritoneal deposits and calcification change.
Conclusions: This preliminary study shows that post-therapy increase in peritoneal implant calcification in low-grade serous ovarian carcinomas is not an indicator of response to therapy.
Keywords: CT scan; Ovarian carcinoma; Tumor marker.
Figures










References
-
- Agarwal A, Yeh BM, Breiman RS, Qayyum A, Coakley FV. Peritoneal calcification: causes and distinguishing features on CT. AJR American journal of roentgenology. 2004;182(2):441–445. doi:10.2214/ajr.182.2.1820441. - PubMed
-
- Hale HL, Husband JE, Gossios K, Norman AR, Cunningham D. CT of calcified liver metastases in colorectal carcinoma. Clinical radiology. 1998;53(10):735–741. - PubMed
-
- Lewis RB, Lattin GE, Jr., Paal E. Pancreatic endocrine tumors: radiologic-clinicopathologic correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2010;30(6):1445–1464. doi:10.1148/rg.306105523. - PubMed
-
- Mc Auley G, Jagannathan J, O'Regan K, Krajewski KM, Hornick JL, Butrynski J, Ramaiya N. Extraskeletal osteosarcoma: spectrum of imaging findings. AJR American journal of roentgenology. 2012;198(1):W31–37. doi:10.2214/ajr.11.6927. - PubMed
-
- Pickhardt PJ, Levy AD, Rohrmann CA, Jr., Kende AI. Primary neoplasms of the appendix: radiologic spectrum of disease with pathologic correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2003;23(3):645–662. doi:10.1148/rg.233025134. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
