

Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base
- PMID: 26970050
- PMCID: PMC4860079
- DOI: 10.1002/cncr.29938
Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base
Abstract
Background: There has been increasing interest in the primary surgical treatment of patients with early T classification (T1-T2) oropharyngeal squamous cell carcinoma (OPSCC), with the stated goal of de-escalating or avoiding adjuvant treatment. Herein, the authors sought to determine the degree to which this interest has translated into changes in practice patterns, and the rates of adverse postoperative pathologic features.
Methods: Patients with T1 to T2 OPSCC in the National Cancer Data Base who were treated from 2004 through 2013 were categorized as receiving primary surgical or primary radiation-based treatment. Trends in treatment selection and factors related to the selection of primary surgery were examined. The rates of adverse pathologic features including positive surgical margins, extracapsular spread (ECS), and advanced T and N classifications after surgery were analyzed.
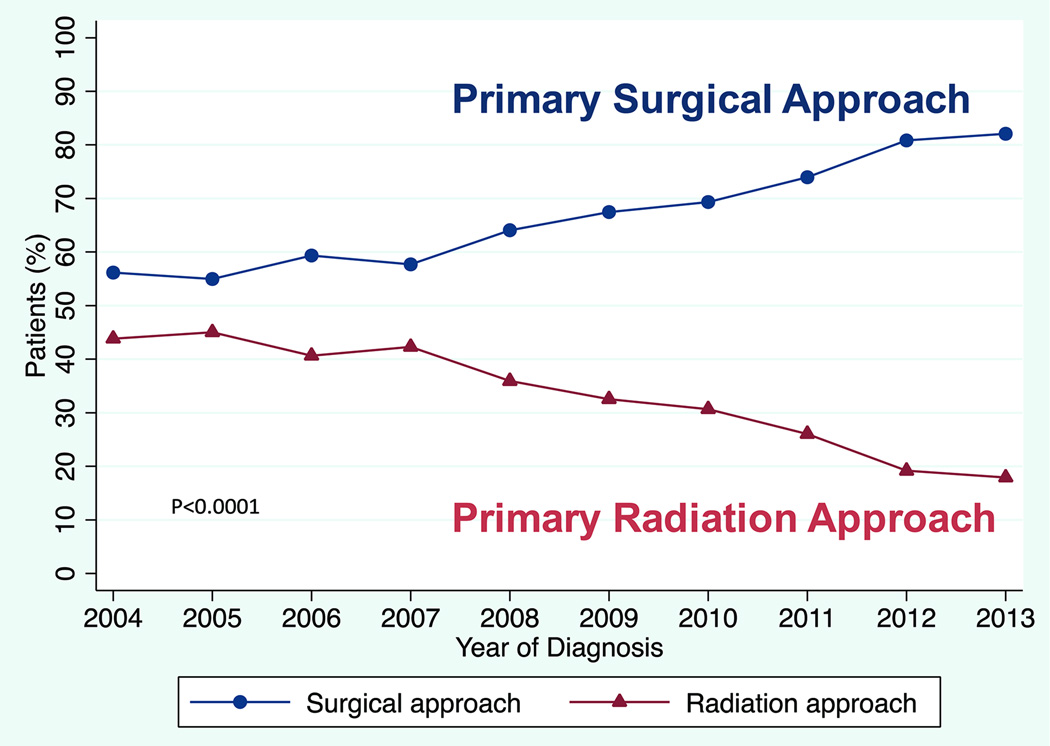
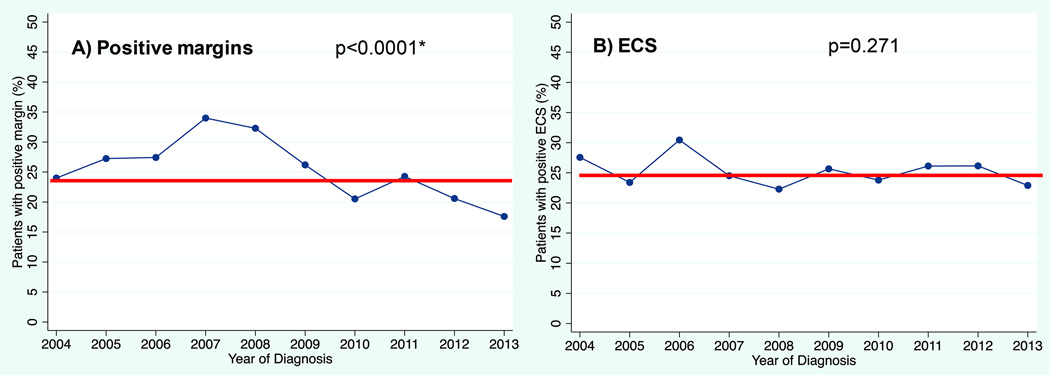
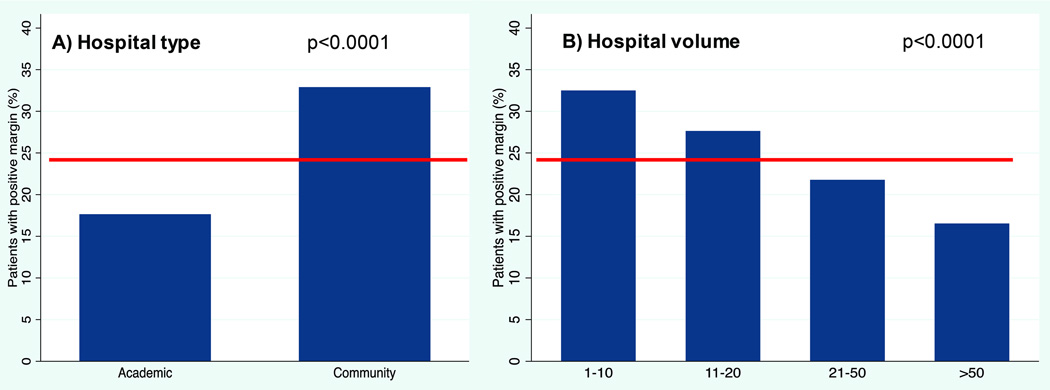
Results: Of 8768 patients with T1 to T2 OPSCC, 68% underwent primary surgical treatment, increasing from 56% in 2004 to 82% in 2013 (P<.0001). The highest versus lowest volume hospitals treated 78% versus 59% of patients with primary surgery (odds ratio, 2.23; 95% confidence interval, 1.55-3.22 [P<.0001]). Higher lymph node classification was found to be predictive of lower rates of primary surgery, but the majority of patients with clinical N2/N3 disease underwent primary surgery. Among patients treated with surgery, positive surgical margins were present in 24% and ECS in 25% of patients. The rate of positive surgical margins decreased over time (P<.0001) and was observed less often at high-volume centers (P<.0001). Among candidates for single-modality therapy (those with clinical T1-T2/N0-N1 disease), 33% had positive surgical margins and/or ECS and 47% had at least 1 adverse feature (T3-T4 disease, N2-N3 disease, positive surgical margins, and/or ECS).
Conclusions: Primary surgical treatment among patients with early T classification OPSCC has become more widespread. Cancer 2016;122:1523-32. © 2016 American Cancer Society.
Keywords: extracapsular spread (ECS); human papillomavirus-related oropharyngeal squamous cell carcinoma (OPSCC); positive surgical margins; transoral robotic surgery (TORS); treatment selection.
© 2016 American Cancer Society.
Conflict of interest statement
Conflict of interest: None (all authors)
Figures

References
-
- D'Souza G, Kreimer AR, Viscidi R, et al. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med. 2007;356(19):1944–1956. - PubMed
-
- Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol. 2008;26(4):612–619. - PubMed
-
- Sedaghat AR, Zhang Z, Begum S, et al. Prognostic significance of human papillomavirus in oropharyngeal squamous cell carcinomas. Laryngoscope. 2009;119(8):1542–1549. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
