

Re-inventing adherence: toward a patient-centered model of care for drug-resistant tuberculosis and HIV
- PMID: 26970149
- PMCID: PMC4863995
- DOI: 10.5588/ijtld.15.0360
Re-inventing adherence: toward a patient-centered model of care for drug-resistant tuberculosis and HIV
Abstract
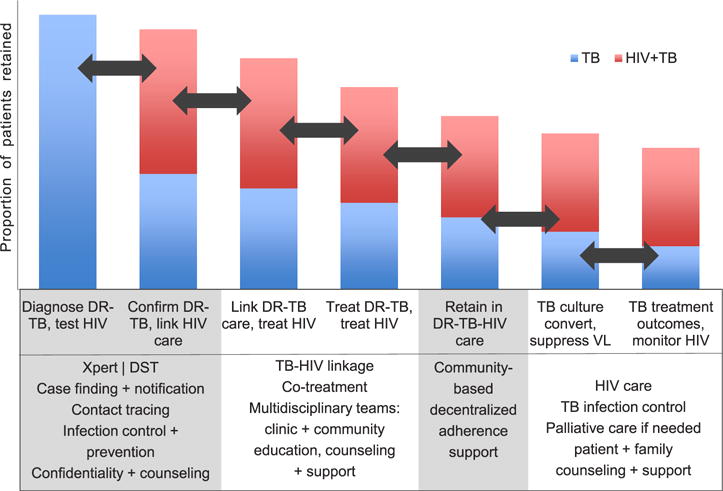
Background: Despite renewed focus on molecular tuberculosis (TB) diagnostics and new antimycobacterial agents, treatment outcomes for patients co-infected with drug-resistant TB and human immunodeficiency virus (HIV) remain dismal, in part due to lack of focus on medication adherence as part of a patient-centered continuum of care.
Objective: To review current barriers to drug-resistant TB-HIV treatment and propose an alternative model to conventional approaches to treatment support.
Discussion: Current national TB control programs rely heavily on directly observed therapy (DOT) as the centerpiece of treatment delivery and adherence support. Medication adherence and care for drug-resistant TB-HIV could be improved by fully implementing team-based patient-centered care, empowering patients through counseling and support, maintaining a rights-based approach while acknowledging the responsibility of health care systems in providing comprehensive care, and prioritizing critical research gaps.
Conclusion: It is time to re-invent our understanding of adherence in drug-resistant TB and HIV by focusing attention on the complex clinical, behavioral, social, and structural needs of affected patients and communities.
Conflict of interest statement
Conflicts of interest: none declared.
Figures
Similar articles
-
[Patient-centered medicine for tuberculosis medical services].Kekkaku. 2012 Dec;87(12):795-808. Kekkaku. 2012. PMID: 23350521 Japanese.
-
Patients infected by tuberculosis and human immunodeficiency virus facing their disease, their reactions to disease diagnosis and its implication about their families and communities, in Burkina Faso: a mixed focus group and cross sectional study.BMC Res Notes. 2016 Jul 29;9:373. doi: 10.1186/s13104-016-2183-3. BMC Res Notes. 2016. PMID: 27473578 Free PMC article.
-
People-centered tuberculosis care versus standard directly observed therapy: study protocol for a cluster randomized controlled trial.Trials. 2015 Jun 22;16:281. doi: 10.1186/s13063-015-0802-2. Trials. 2015. PMID: 26093675 Free PMC article. Clinical Trial.
-
An integrated review of directly observed therapy for tuberculosis in Latin America.Hisp Health Care Int. 2015;13(1):46-54. doi: 10.1891/1540-4153.13.1.46. Hisp Health Care Int. 2015. PMID: 25741933 Review.
-
Predictors of cure among HIV co-infected multidrug-resistant TB patients at Sizwe Tropical Disease Hospital Johannesburg, South Africa.Trans R Soc Trop Med Hyg. 2015 May;109(5):340-8. doi: 10.1093/trstmh/trv025. Epub 2015 Mar 18. Trans R Soc Trop Med Hyg. 2015. PMID: 25787727 Review.
Cited by
-
Preparing the healthcare workforce in South Africa for short-course rifampicin-resistant TB treatment: inter-professional training and task-sharing considerations.Hum Resour Health. 2021 Jan 6;19(1):6. doi: 10.1186/s12960-020-00552-1. Hum Resour Health. 2021. PMID: 33407541 Free PMC article.
-
Effect of Curcumin in Experimental Pulmonary Tuberculosis: Antimycobacterial Activity in the Lungs and Anti-Inflammatory Effect in the Brain.Int J Mol Sci. 2022 Feb 10;23(4):1964. doi: 10.3390/ijms23041964. Int J Mol Sci. 2022. PMID: 35216083 Free PMC article.
-
Global, regional, and national burden of tuberculosis, 1990-2016: results from the Global Burden of Diseases, Injuries, and Risk Factors 2016 Study.Lancet Infect Dis. 2018 Dec;18(12):1329-1349. doi: 10.1016/S1473-3099(18)30625-X. Lancet Infect Dis. 2018. PMID: 30507459 Free PMC article.
-
Role Of Vitamin-D Supplementation In TB/HIV Co-Infected Patients.Infect Drug Resist. 2020 Jan 10;13:111-118. doi: 10.2147/IDR.S228336. eCollection 2020. Infect Drug Resist. 2020. PMID: 32021325 Free PMC article. Review.
-
Risk factors for tuberculosis smear non-conversion in Eden district, Western Cape, South Africa, 2007-2013: a retrospective cohort study.BMC Infect Dis. 2016 Aug 2;16:365. doi: 10.1186/s12879-016-1712-y. BMC Infect Dis. 2016. PMID: 27484399 Free PMC article.
References
-
- World Health Organization. Global tuberculosis report, 2014. Geneva, Switzerland: WHO; 2014. (WHO/HTM/TB/2014.08).
-
- World Health Organization. Towards universal access to diagnosis and treatment of multidrug-resistant and extensively drug-resistant tuberculosis by 2015: WHO progress report. Geneva, Switzerland: WHO; 2011. (WHO/HTM/TB/2011.3). http://www.who.int/tb/publications/2011/mdr_report_2011/en/. Accessed December 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
