

The Association of Coronary Artery Calcium With Noncardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis
- PMID: 26970999
- PMCID: PMC4860157
- DOI: 10.1016/j.jcmg.2015.09.020
The Association of Coronary Artery Calcium With Noncardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis
Abstract
Objectives: This study sought to determine if coronary artery calcium (CAC) is associated with incident noncardiovascular disease.
Background: CAC is considered a measure of vascular aging, associated with increased risk of cardiovascular and all-cause mortality. The relationship with noncardiovascular disease is not well defined.
Methods: A total of 6,814 participants from 6 MESA (Multi-Ethnic Study of Atherosclerosis) field centers were followed for a median of 10.2 years. Modified Cox proportional hazards ratios accounting for the competing risk of fatal coronary heart disease were calculated for new diagnoses of cancer, pneumonia, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), deep vein thrombosis/pulmonary embolism, hip fracture, and dementia. Analyses were adjusted for age; sex; race; socioeconomic status; health insurance status; body mass index; physical activity; diet; tobacco use; number of medications used; systolic and diastolic blood pressure; total and high-density lipoprotein cholesterol; antihypertensive, aspirin, and cholesterol medication; and diabetes. The outcome was first incident noncardiovascular disease diagnosis.
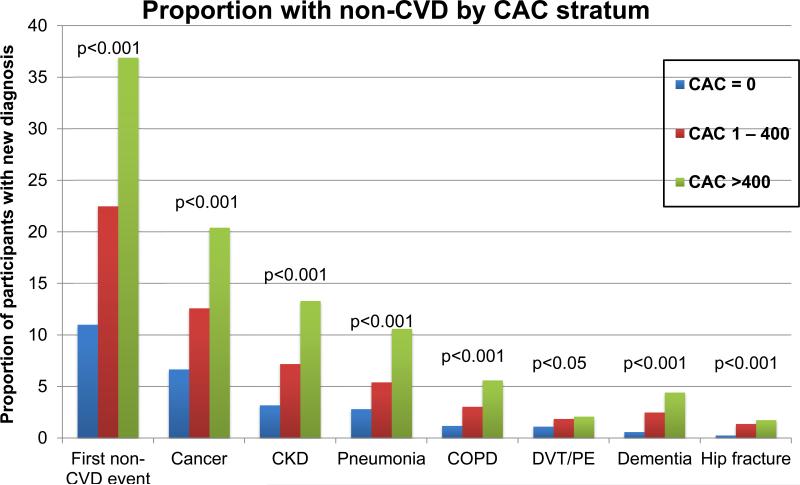
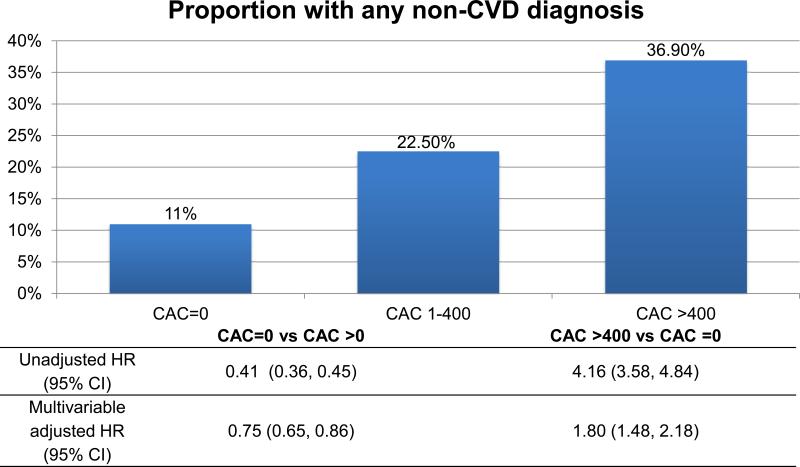
Results: Compared with those with CAC = 0, those with CAC >400 had an increased hazard of cancer (hazard ratio [HR]: 1.53; 95% confidence interval [CI]: 1.18 to 1.99), CKD (HR: 1.70; 95% CI: 1.21 to 2.39), pneumonia (HR: 1.97; 95% CI: 1.37 to 2.82), COPD (HR: 2.71; 95% CI: 1.60 to 4.57), and hip fracture (HR: 4.29; 95% CI: 1.47 to 12.50). CAC >400 was not associated with dementia or deep vein thrombosis/pulmonary embolism. Those with CAC = 0 had decreased risk of cancer (HR: 0.76; 95% CI: 0.63 to 0.92), CKD (HR: 0.77; 95% CI: 0.60 to 0.98), COPD (HR: 0.61; 95% CI: 0.40 to 0.91), and hip fracture (HR: 0.31; 95% CI: 0.14 to 0.70) compared to those with CAC >0. CAC = 0 was not associated with less pneumonia, dementia, or deep vein thrombosis/pulmonary embolism. The results were attenuated, but remained significant, after removing participants developing interim nonfatal coronary heart disease.
Conclusions: Participants with elevated CAC were at increased risk of cancer, CKD, COPD, and hip fractures. Those with CAC = 0 are less likely to develop common age-related comorbid conditions, and represent a unique population of "healthy agers."
Keywords: aging; biologic aging; cancer; coronary artery calcium; coronary artery disease.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Imaging Atherosclerosis for Global Predictive Health and Wellness.JACC Cardiovasc Imaging. 2016 May;9(5):577-9. doi: 10.1016/j.jcmg.2015.09.021. Epub 2016 Mar 9. JACC Cardiovasc Imaging. 2016. PMID: 26970998 No abstract available.
References
-
- Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356:2388–98. - PubMed
-
- Araujo F, Gouvinhas C, Fontes F, La Vecchia C, Azevedo A, Lunet N. Trends in cardiovascular diseases and cancer mortality in 45 countries from five continents (1980-2010). Eur J Prev Cardiol. 2013 - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics for hispanics/latinos, 2012. CA Cancer J Clin. 2012;62:283–98. - PubMed
-
- Shaw LJ, Raggi P, Schisterman E, Berman DS, Callister TQ. Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology. 2003;228:826–33. - PubMed
-
- McClelland RL, Chung H, Detrano R, Post W, Kronmal RA. Distribution of coronary artery calcium by race, gender, and age: Results from the multi-ethnic study of atherosclerosis (MESA). Circulation. 2006;113:30–7. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- L30 HL110027/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical