

High Prevalence and Heterogeneity of Diabetes in Patients With TB in South India: A Report from the Effects of Diabetes on Tuberculosis Severity (EDOTS) Study
- PMID: 26973015
- PMCID: PMC4944775
- DOI: 10.1016/j.chest.2016.02.675
High Prevalence and Heterogeneity of Diabetes in Patients With TB in South India: A Report from the Effects of Diabetes on Tuberculosis Severity (EDOTS) Study
Abstract
Background: Previous studies reported an association of diabetes mellitus (DM) with TB susceptibility. Many studies were retrospective, had weak diagnostic criteria for DM, and did not assess other comorbidities. The Effects of Diabetes on Tuberculosis Severity (EDOTS) study is addressing these limitations with a longitudinal comparison of patients with TB who are classified as diabetic or normoglycemic according to World Health Organization criteria. We report interim findings after enrolling 159 of a planned 300 subjects.
Methods: A cohort study of patients with TB in South India with DM or normoglycemia defined by oral glucose tolerance test (OGTT) and fasting glucose. Glycohemoglobin (HbA1c), serum creatinine, lipids, and 25-hydroxyvitamin D were measured at enrollment. Patients were monitored monthly during TB treatment, and HbA1c measurement was repeated after 3 months.
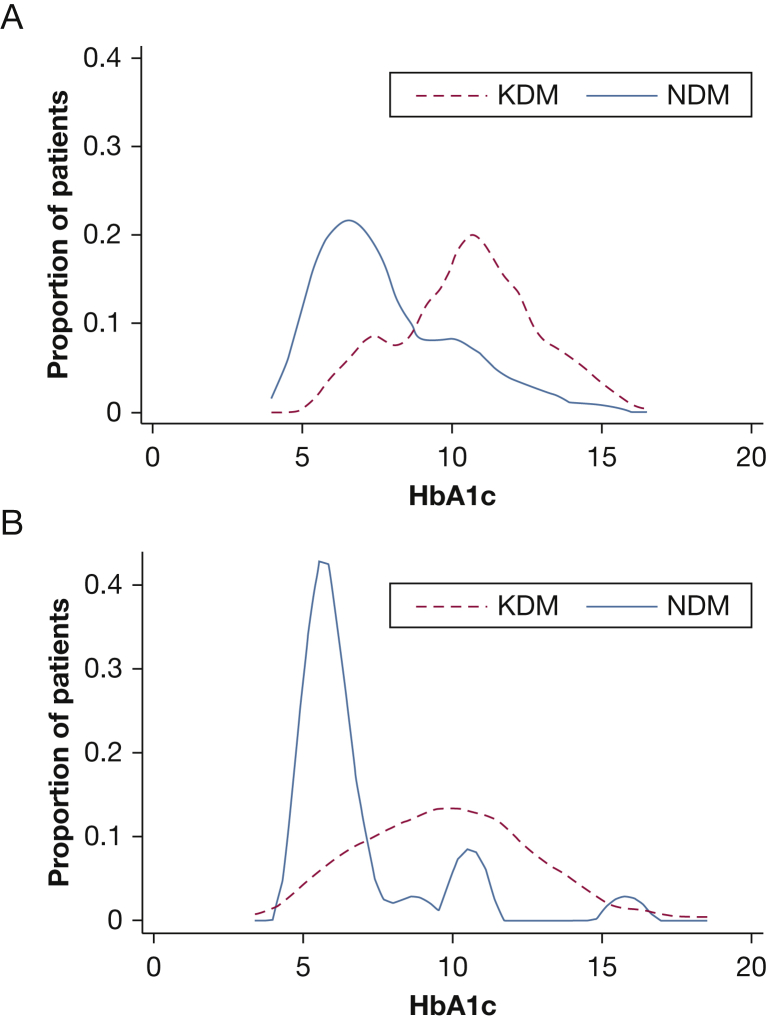
Results: Of 209 eligible patients, 113 (54.1%) were classified as diabetic, 44 (21.0%) with impaired glucose tolerance, and 52 (24.9%) as normoglycemic. More patients with diabetes were detected by OGTT than by HbA1c. Diabetes was a newly received diagnosis for 37 (32.7%) in the DM group, and their median HbA1c (6.8%) was significantly lower than in those with previously diagnosed DM (HbA1c, 10.4%). Among 129 patients monitored for 3 months, HbA1c declined in all groups, with the greatest difference in patients with a newly received diagnosis of DM.
Conclusions: Early EDOTS study results reveal a strikingly high prevalence of glycemic disorders in South Indian patients with pulmonary TB and unexpected heterogeneity within the patient population with diabetes and TB. This glycemic control heterogeneity has implications for the TB-DM interaction and the interpretation of TB studies relying exclusively on HbA1c to define diabetic status.
Keywords: chest imaging; diabetes; global medicine; tuberculosis.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Chen L., Magliano D.J., Zimmet P.Z. The worldwide epidemiology of type 2 diabetes mellitus—present and future perspectives. Nat Rev Endocrinol. 2012;8(4):228–236. - PubMed
-
- World Health Organization . WHO Press; Geneva: 2014. Global Tuberculosis Report 2014.
-
- Odone A., Houben R.M., White R.G. The effect of diabetes and undernutrition trends on reaching 2035 global tuberculosis targets. Lancet Diabetes Endocrinol. 2014;2(9):754–764. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
