

A novel ciprofloxacin-resistant subclade of H58 Salmonella Typhi is associated with fluoroquinolone treatment failure
- PMID: 26974227
- PMCID: PMC4805543
- DOI: 10.7554/eLife.14003
A novel ciprofloxacin-resistant subclade of H58 Salmonella Typhi is associated with fluoroquinolone treatment failure
Abstract
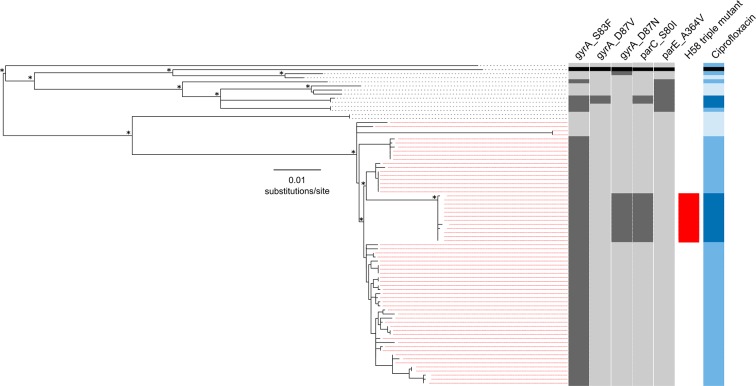
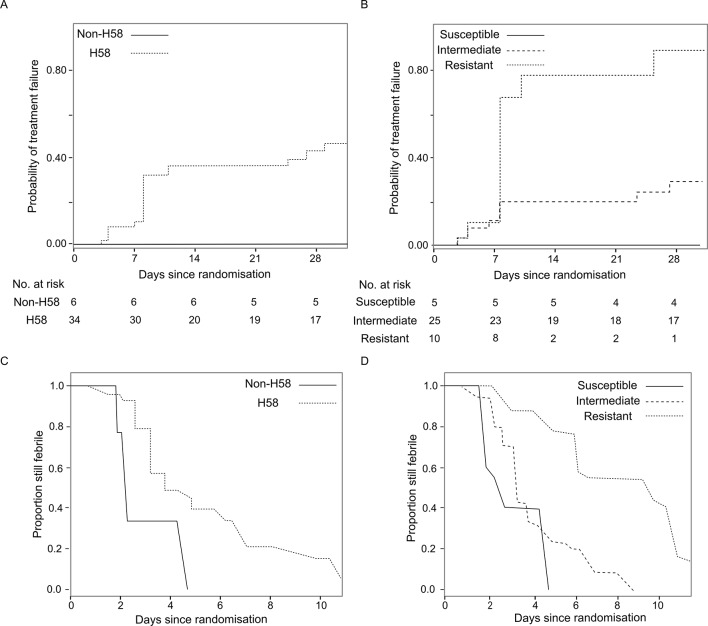
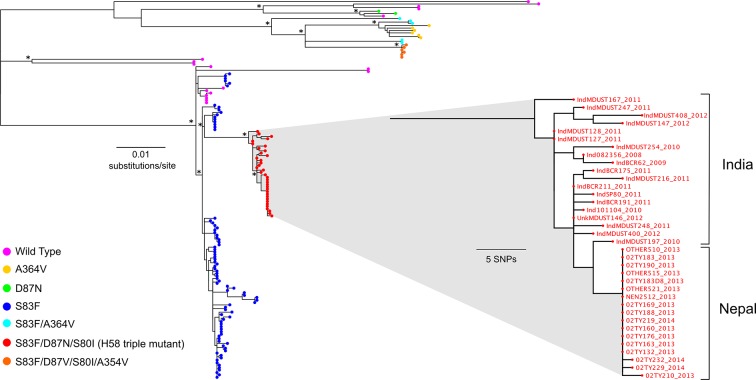
The interplay between bacterial antimicrobial susceptibility, phylogenetics and patient outcome is poorly understood. During a typhoid clinical treatment trial in Nepal, we observed several treatment failures and isolated highly fluoroquinolone-resistant Salmonella Typhi (S. Typhi). Seventy-eight S. Typhi isolates were genome sequenced and clinical observations, treatment failures and fever clearance times (FCTs) were stratified by lineage. Most fluoroquinolone-resistant S. Typhi belonged to a specific H58 subclade. Treatment failure with S. Typhi-H58 was significantly less frequent with ceftriaxone (3/31; 9.7%) than gatifloxacin (15/34; 44.1%)(Hazard Ratio 0.19, p=0.002). Further, for gatifloxacin-treated patients, those infected with fluoroquinolone-resistant organisms had significantly higher median FCTs (8.2 days) than those infected with susceptible (2.96) or intermediately resistant organisms (4.01)(pS. Typhi clade internationally, but there are no data regarding disease outcome with this organism. We report an emergent new subclade of S. Typhi-H58 that is associated with fluoroquinolone treatment failure.
Keywords: s. enterica serovar typhi; H58; epidemiology; fluoroquinolones; global health; human; infectious disease; microbiology; nepal; randomised controlled trial; treatment failure; typhoid fever.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures
References
-
- Arjyal A, Basnyat B, Koirala S, Karkey A, Dongol S, Agrawaal KK, Shakya N, Shrestha K, Sharma M, Lama S, Shrestha K, Khatri NS, Shrestha U, Campbell JI, Baker S, Farrar J, Wolbers M, Dolecek C. Gatifloxacin versus chloramphenicol for uncomplicated enteric fever: an open-label, randomised, controlled trial. The Lancet Infectious Diseases. 2011;11:445–454. doi: 10.1016/S1473-3099(11)70089-5. - DOI - PMC - PubMed
-
- Arjyal A, Basnyat B, Nhan HT, Koirala S, Giri A, Joshi N, Shakya M, Pathak KR, Mahat SP, Prajapati SP, Adhikari N, Thapa R, Merson L, Gajurel D, Lamsal K, Lamsal D, Yadav BK, Shah G, Shrestha P, Dongol S, Karkey A, Thompson CN, Thieu NTV, Thanh DP, Baker S, Thwaites GE, Wolbers M, Dolecek C. Gatifloxacin versus ceftriaxone for uncomplicated enteric fever in nepal: an open-label, two-centre, randomised controlled trial. The Lancet Infectious Diseases. 2016 doi: 10.1016/S1473-3099(15)00530-7. - DOI - PMC - PubMed
-
- CLSI Clinical and laboratory standards institute: performance standards for antimicrobial susceptibility testing. Twentieth Informational Supplement. 2012:M100–S22.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
