

Distinct Clinical Characteristics of Pediatric Guillain-Barré Syndrome: A Comparative Study between Children and Adults in Northeast China
- PMID: 26974666
- PMCID: PMC4790924
- DOI: 10.1371/journal.pone.0151611
Distinct Clinical Characteristics of Pediatric Guillain-Barré Syndrome: A Comparative Study between Children and Adults in Northeast China
Abstract
Objective: Clinical characteristics of pediatric Guillain-Barré syndrome (GBS) have been extensively studied whereas scarcely been compared with those of adult GBS. Herein we compared the clinical features of GBS between pediatric and adult patients.
Methods: We retrospectively collected the clinical data of 750 patients with GBS (541 adults and 209 children), and compared the clinical characteristics between children and adults.
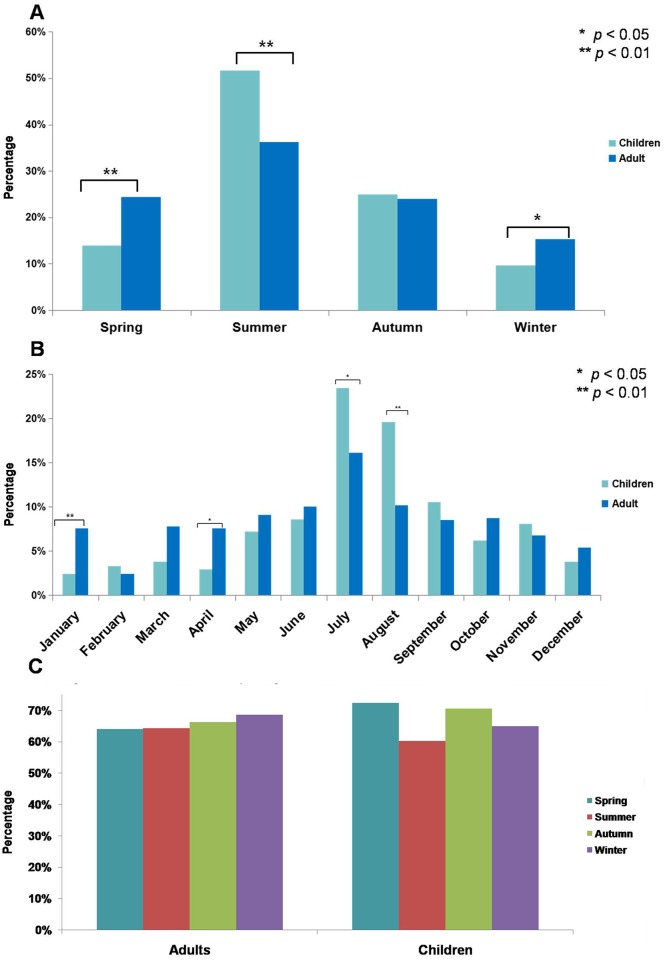
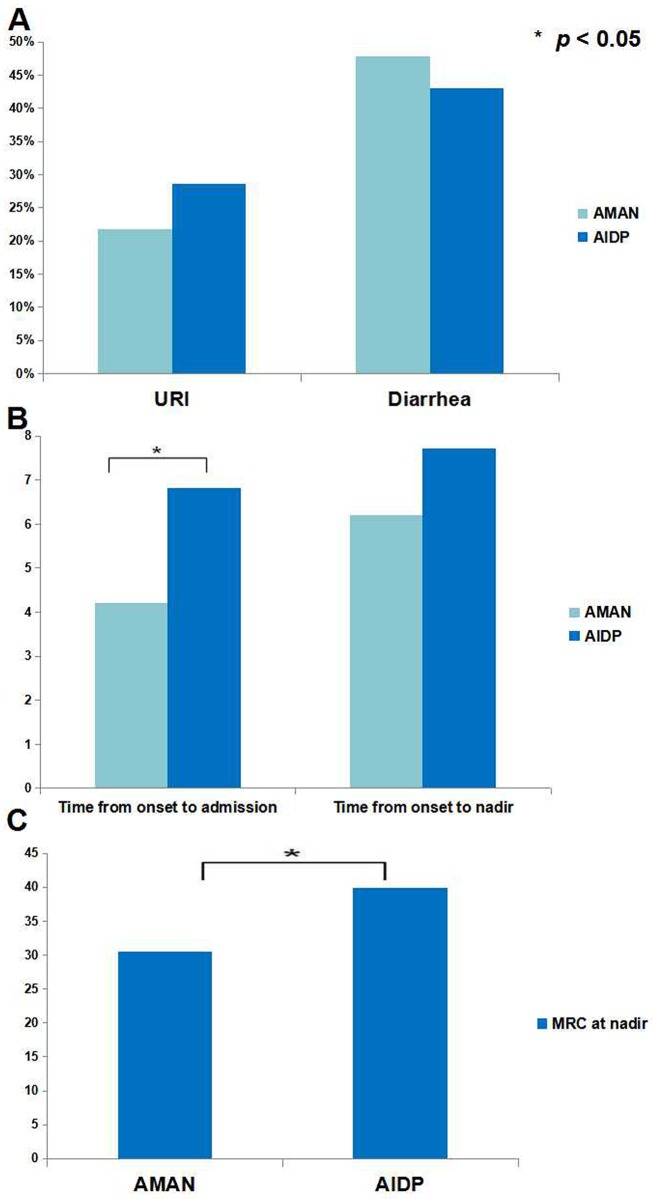
Results: Pain was a more frequent complaint in children (17.2% vs 9.6%, p < 0.01), who were also found with shorter interval from disease onset to nadir (6.3d vs 7.3d, p < 0.01) and higher incidence of bulbar dysfunction (22.0% vs 14.8%, p < 0.05). The disease severity in children was comparable with adults. In addition, a higher incidence of pediatric GBS was found in summer, especially in July and August (both p < 0.01). However, the incidence of antecedent infections of different seasons in adult and pediatric patients was comparable (p > 0.05). The clinical features of acute motor axonal neuropathy (AMAN) and acute inflammatory demyelinating polyneuropathy (AIDP) in children were overall comparable with adult ones (p > 0.05). Similar to adults, bulbar dysfunction (odds ratio [OR]: 4.621, 95% confidence interval [CI]: 1.240-17.218, p < 0.05) and lower nadir Medical Research Council (MRC) sum score (OR: 0.897, 95% CI: 0.855-0.941, p < 0.01) were also risk factors for mechanical ventilation in children. However, distinct from adult ones, autonomic dysfunction was significantly higher in mechanically ventilated childhood GBS (39.1% vs 8.8%, p < 0.01), which also served as a predictor for mechanical ventilation in pediatric GBS (OR: 70.415, 95% CI: 9.265-535.158, p < 0.01). As to the efficacy of intravenous immunoglobulin, insignificant difference was identified between children and adults.
Conclusion: The clinical features of pediatric GBS differ from those of adults. Autonomic dysfunction is an independent risk factor for mechanical ventilation in pediatric patients.
Conflict of interest statement
Figures
Similar articles
-
Predictors for mechanical ventilation and short-term prognosis in patients with Guillain-Barré syndrome.Crit Care. 2015 Sep 2;19(1):310. doi: 10.1186/s13054-015-1037-z. Crit Care. 2015. PMID: 26330143 Free PMC article.
-
Clinico-electrophysiological profile and predictors of functional outcome in Guillain-Barre syndrome (GBS).J Neurol Sci. 2013 Dec 15;335(1-2):105-11. doi: 10.1016/j.jns.2013.09.002. Epub 2013 Sep 10. J Neurol Sci. 2013. PMID: 24064258
-
Clinical and electrophysiologic features of childhood Guillain-Barré syndrome in Northeast China.J Formos Med Assoc. 2014 Sep;113(9):634-9. doi: 10.1016/j.jfma.2012.08.011. Epub 2012 Sep 8. J Formos Med Assoc. 2014. PMID: 25103077
-
Guillain-Barré syndrome: epidemiology, pathophysiology and management.Drugs. 2004;64(6):597-610. doi: 10.2165/00003495-200464060-00003. Drugs. 2004. PMID: 15018590 Review.
-
Diagnosis, treatment and prognosis of Guillain-Barré syndrome (GBS).Presse Med. 2013 Jun;42(6 Pt 2):e193-201. doi: 10.1016/j.lpm.2013.02.328. Epub 2013 Apr 28. Presse Med. 2013. PMID: 23628447 Review.
Cited by
-
Epidemiology of Guillain-Barré Syndrome in Iranian Children Aged 0-15 Years (2008-2013).Iran J Child Neurol. 2021 Fall;15(4):27-34. doi: 10.22037/ijcn.v15i4.25087. Iran J Child Neurol. 2021. PMID: 34782839 Free PMC article.
-
Clinical characteristics and functional outcomes of pediatric Guillain-Barré syndrome admitted to the Neuro-intensive care unit: a decade-long retrospective observational study.Neurol Sci. 2025 Mar;46(3):1369-1377. doi: 10.1007/s10072-024-07862-5. Epub 2024 Nov 7. Neurol Sci. 2025. PMID: 39505753
-
Clinico-epidemiological profile and prediction of outcome in children with Guillain-Barre syndrome.Ital J Pediatr. 2025 Jun 7;51(1):179. doi: 10.1186/s13052-025-02037-0. Ital J Pediatr. 2025. PMID: 40483522 Free PMC article.
-
Hyperreflexia and Preserved Reflexes in Pediatric Guillain-Barré Syndrome: A Case Report and Literature Review.Cureus. 2025 Jun 1;17(6):e85172. doi: 10.7759/cureus.85172. eCollection 2025 Jun. Cureus. 2025. PMID: 40600102 Free PMC article.
-
Serial Serum Immunoglobulin G Levels and Correlation with Outcomes in Children with Guillain Barre Syndrome.Indian J Pediatr. 2025 Jun 26. doi: 10.1007/s12098-025-05633-4. Online ahead of print. Indian J Pediatr. 2025. PMID: 40569328
References
-
- Ryan MM. Guillain-Barré syndrome in childhood. J Paediatr Child Health. 2005; 41: 237–41. - PubMed
-
- Nachamkin I, Arzarte Barbosa P, Ung H, Lobato C, Gonzalez Rivera A, Rodriguez P, et al. Patterns of Guillain-Barre syndrome in children: results from a Mexican population. Neurology. 2007; 69: 1665–71. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
