

The influence of clinical and genetic factors on patient outcome in small cell carcinoma of the ovary, hypercalcemic type
- PMID: 26975901
- PMCID: PMC6876126
- DOI: 10.1016/j.ygyno.2016.03.013
The influence of clinical and genetic factors on patient outcome in small cell carcinoma of the ovary, hypercalcemic type
Abstract
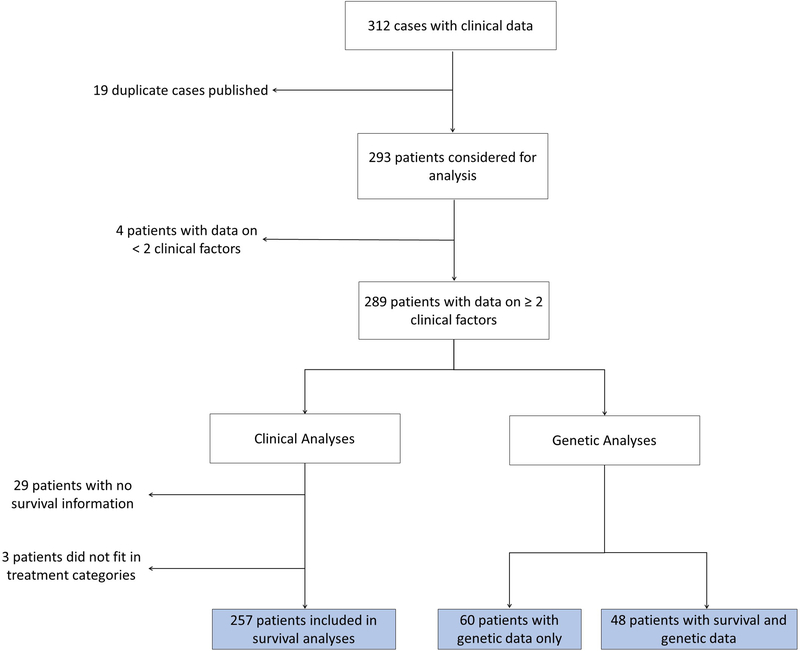
Objective: Small cell carcinoma of the ovary, hypercalcemic type (SCCOHT) is an aggressive tumor, with long term survival at ~30% in early stage disease. SCCOHT is caused by germline and somatic SMARCA4 mutations, but the effect of the mutation type on patients remains unknown. Furthermore, the rarity of SCCOHT has resulted in varied treatment, with no standardized protocols. We analyzed 293 cases to determine the effect of treatment modalities and SMARCA4 mutations on patient diagnosis and outcome.
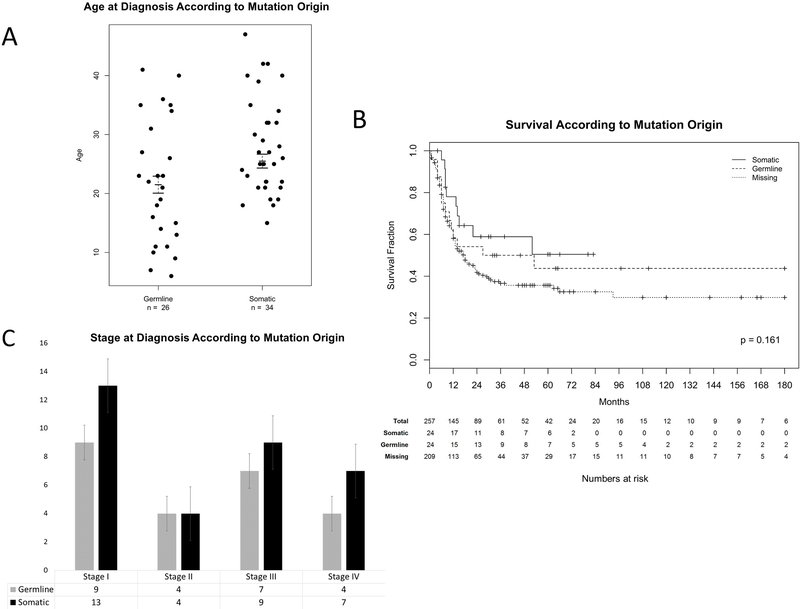
Methods: In 293 SCCOHT patients we collected information on age and stage at diagnosis, treatment modality (surgery, chemotherapy, radiotherapy, and/or high-dose chemotherapy with autologous stem cell rescue (HDC-aSCR)), SMARCA4 mutation origin (germline/somatic), and overall survival. Cox analysis and log-rank tests were performed on 257 cases with available survival data.
Results: The strongest prognostic factors were stage at diagnosis (p=2.72e-15) and treatment modality (p=3.87e-13). For FIGO stages II-IV, 5-year survival was 71% for patients who received HDC-aSCR, compared to 25% in patients who received conventional chemotherapy alone following surgery (p=0.002). Patients aged ≥40 had a worse outcome than younger patients (p=0.04). Twenty-six of 60 tested patients carried a germline SMARCA4 mutation, including all patients diagnosed <15years; carriers presented at a younger age than non-carriers (p=0.02).
Conclusions: Stage at diagnosis is the most significant prognostic factor in SCCOHT and consolidation with HDC-aSCR may provide the best opportunity for long-term survival. The large fraction of SMARCA4 germline mutations carriers warrants genetic counseling for all patients.
Keywords: Chemotherapy; Mutation; Ovarian cancer; SCCOHT; SMARCA4; Stem cell rescue.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures

References
-
- Scully RE. Tumors of the ovary and maldeveloped gonads In: Hartmann WH, Cowan WR, editors. Atlas of Tumor Pathology. second series, fascicle 16 ed. Washington, DC: Armed Forces Institute of Pathology; 1979.
-
- Estel R, Hackethal A, Kalder M, Münstedt K. Small cell carcinoma of the ovary of the hypercalcaemic type: an analysis of clinical and prognostic aspects of a rare disease on the basis of cases published in the literature. Arch Gynecol Obstet. 2011;284(5):1277–82. - PubMed
-
- Jamy O, Yaghmour G, Hare F, Martin MG. Population-based Analysis of the Clinical Features of Primary Small Cell Carcinoma of the Ovary. Anticancer Res. 2015;35(5):3091–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
