

Conventional versus rapid-deployment aortic valve replacement: a single-centre comparison between the Edwards Magna valve and its rapid-deployment successor
- PMID: 26976130
- PMCID: PMC4986793
- DOI: 10.1093/icvts/ivw052
Conventional versus rapid-deployment aortic valve replacement: a single-centre comparison between the Edwards Magna valve and its rapid-deployment successor
Abstract
Objectives: Sutureless and rapid-deployment valves were recently introduced into clinical practice. The Edwards INTUITY valve system is a combination of the Edwards Magna pericardial valve and a subvalvular stent-frame to enable rapid deployment. We performed a parallel cohort study for comparison of the two valve types.
Methods: All patients receiving either an Edwards Magna Ease valve or an Edwards INTUITY valve system due to aortic stenosis from May 2010 until July 2014 were included. Patients undergoing bypass surgery, an additional valve procedure, atrial ablation surgery or replacement of the ascending aorta were excluded. Preoperative characteristics, operative specifications, survival, valve-related adverse events and transvalvulvar gradients were compared.
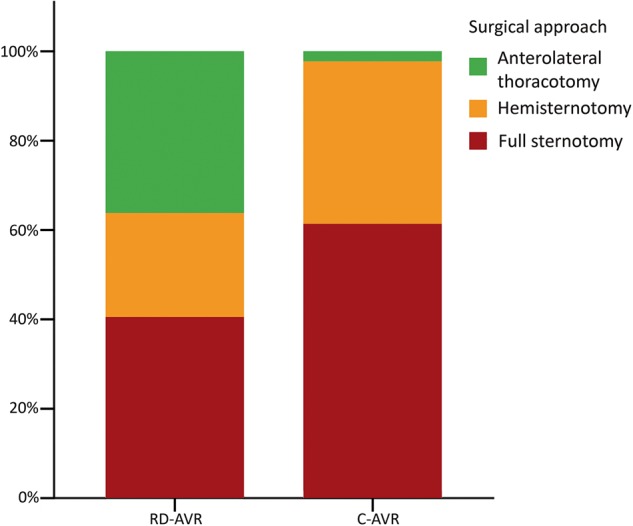
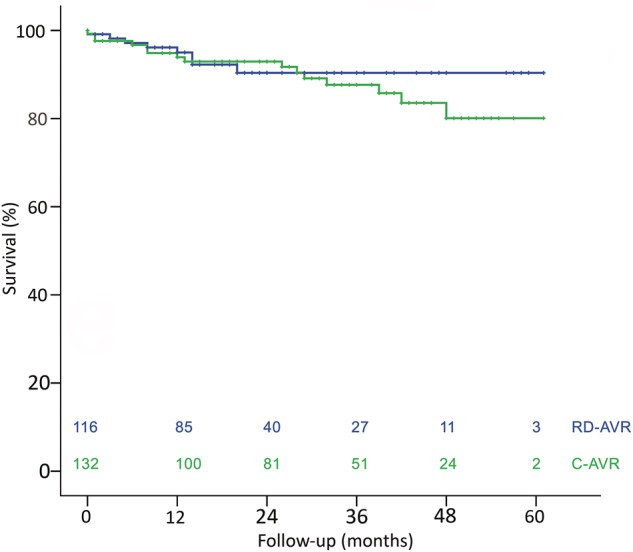
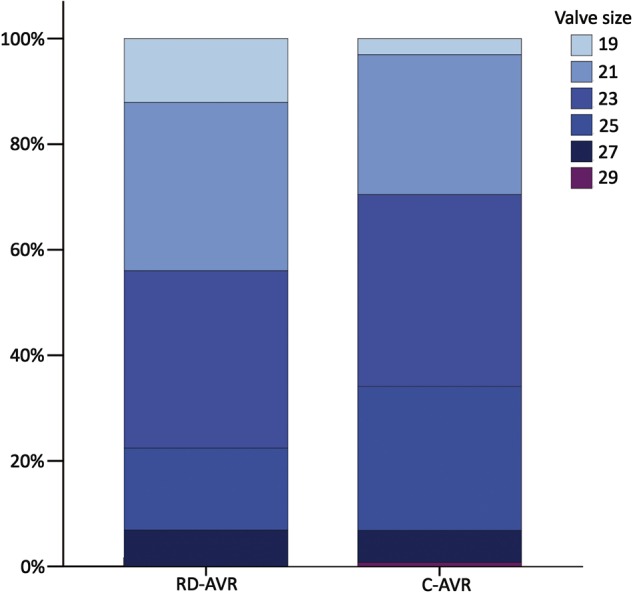
Results: One hundred sixteen patients underwent rapid-deployment aortic valve replacement [mean age 75 years (SD: 8); 62% female] and 132 patients underwent conventional aortic valve replacement [70 years (SD: 9); 31% female; P < 0.001]. Conventional valve patients were taller and heavier. The mean EuroSCORE II was 3.1% (SD: 2.7) and 4.4% (SD: 6.0) for rapid-deployment and conventional valve patients, respectively (P = 0.085). The mean implanted valve size was higher in the conventional group [23.2 mm (SD: 2.0) vs 22.5 mm (SD: 2.2); P = 0.007], but postoperative transvalvular mean gradients were comparable [15 mmHg (SD: 6) vs 14 mmHg (SD: 5); P = 0.457]. A subgroup analysis of the most common valve sizes (21 and 23 mm; implanted in 63% of patients) revealed significantly reduced mean postoperative transvalvular gradients in the rapid-deployment group [14 mmHg (SD: 4) vs 16 mmHg (SD: 5); P = 0.025]. A significantly higher percentage received minimally invasive procedures in the rapid-deployment group (59 vs 39%; P < 0.001). The 1- and 3-year survival rate was 96 and 90% in the rapid-deployment group and 95 and 89% in the conventional group (P = 0.521), respectively. Valve-related pacemaker implantations were more common in the rapid-deployment group (9 vs 2%; P = 0.014) and postoperative stroke was more common in the conventional group (1.6 vs 0% per patient year; P = 0.044).
Conclusions: We conclude that this rapid-deployment valve probably facilitates minimally invasive surgery. Furthermore, a subgroup analysis showed reduced transvalvular gradients in smaller valve sizes compared with the conventionally implanted valve of the same type. The favourable haemodynamic profile and the potentially different spectrum of valve-related adverse events should be addressed in further clinical trials.
Keywords: Aortic valve replacement; Minimally invasive surgery; Rapid deployment; Sutureless valve; Transvalvular gradient.
© The Author 2016. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures
References
-
- Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H et al. . Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg 2012;42:S1–44. - PubMed
-
- Andreas M, Wiedemann D, Seebacher G, Rath C, Aref T, Rosenhek R et al. . The Ross procedure offers excellent survival compared with mechanical aortic valve replacement in a real-world setting. Eur J Cardiothorac Surg 2014;46:409–13; discussion 13–4. - PubMed
-
- Forcillo J, Pellerin M, Perrault LP, Cartier R, Bouchard D, Demers P et al. . Carpentier-Edwards pericardial valve in the aortic position: 25-years experience. Ann Thorac Surg 2013;96:486–93. - PubMed
-
- Cosgrove DM III, Sabik JF. Minimally invasive approach for aortic valve operations. Ann Thorac Surg 1996;62:596–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
