

Phase II Randomized Preoperative Window-of-Opportunity Study of the PI3K Inhibitor Pictilisib Plus Anastrozole Compared With Anastrozole Alone in Patients With Estrogen Receptor-Positive Breast Cancer
- PMID: 26976426
- PMCID: PMC6075966
- DOI: 10.1200/JCO.2015.63.9179
Phase II Randomized Preoperative Window-of-Opportunity Study of the PI3K Inhibitor Pictilisib Plus Anastrozole Compared With Anastrozole Alone in Patients With Estrogen Receptor-Positive Breast Cancer
Abstract
Purpose: Preclinical data support a key role for the PI3K pathway in estrogen receptor-positive breast cancer and suggest that combining PI3K inhibitors with endocrine therapy may overcome resistance. This preoperative window study assessed whether adding the PI3K inhibitor pictilisib (GDC-0941) can increase the antitumor effects of anastrozole in primary breast cancer and aimed to identify the most appropriate patient population for combination therapy.
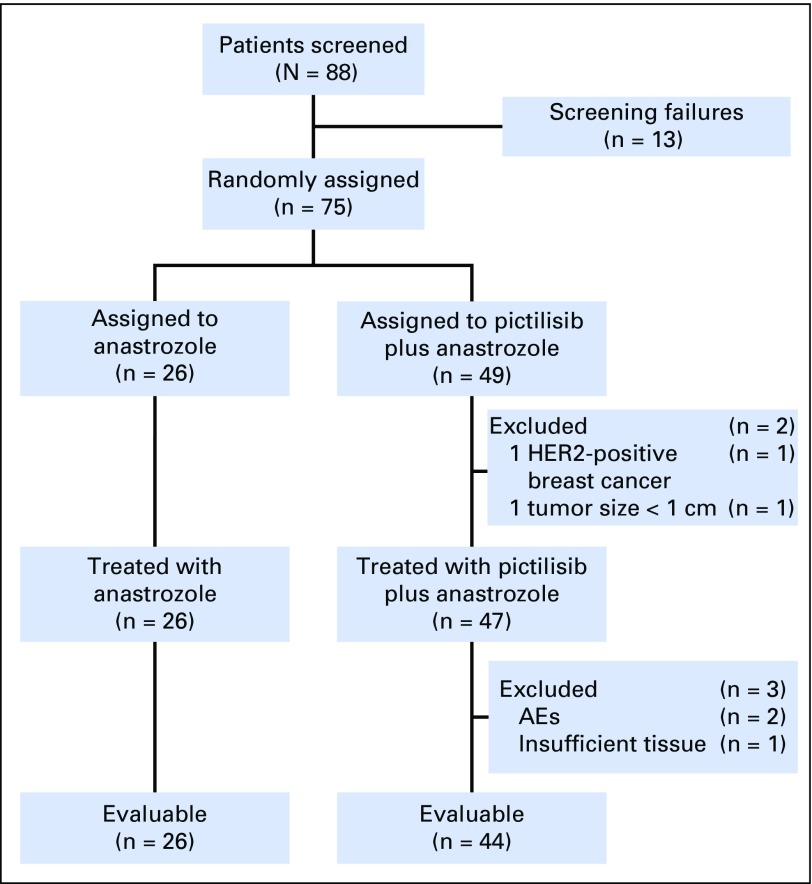
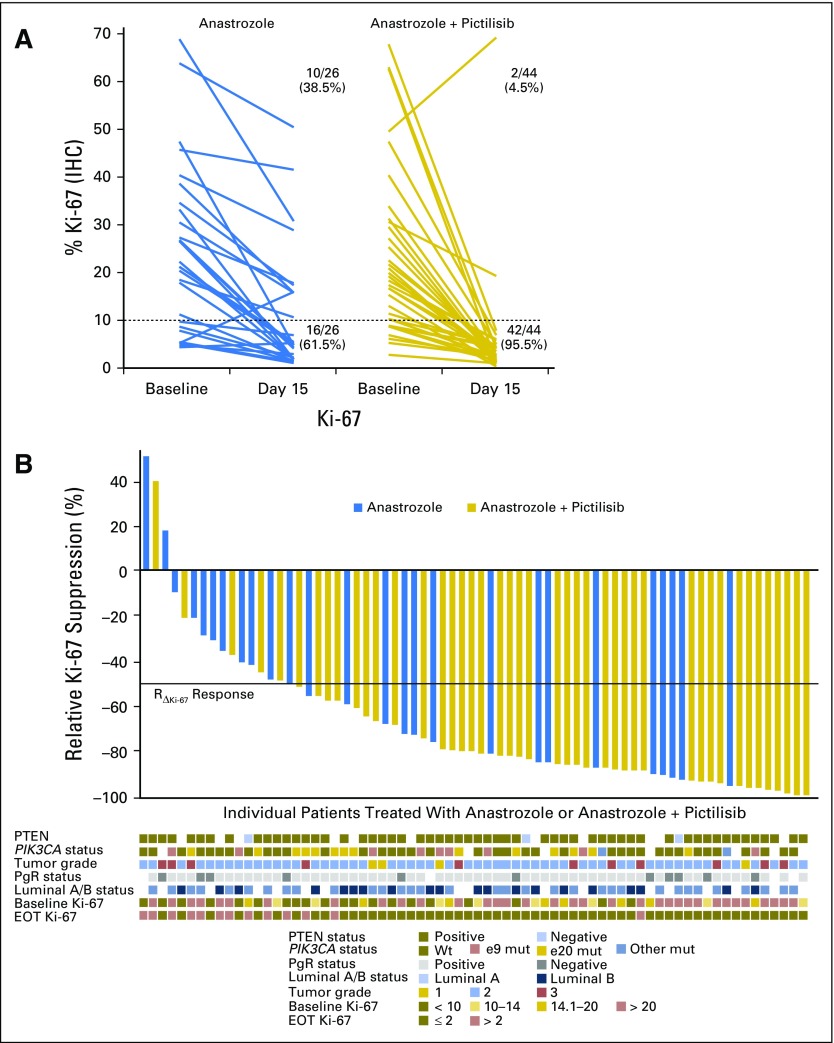
Patients and methods: In this randomized, open-label phase II trial, postmenopausal women with newly diagnosed operable estrogen receptor-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancers were recruited. Participants were randomly allocated (2:1, favoring the combination) to 2 weeks of preoperative treatment with anastrozole 1 mg once per day (n = 26) or the combination of anastrozole 1 mg with pictilisib 260 mg once per day (n = 49). The primary end point was inhibition of tumor cell proliferation as measured by change in Ki-67 protein expression between tumor samples taken before and at the end of treatment.
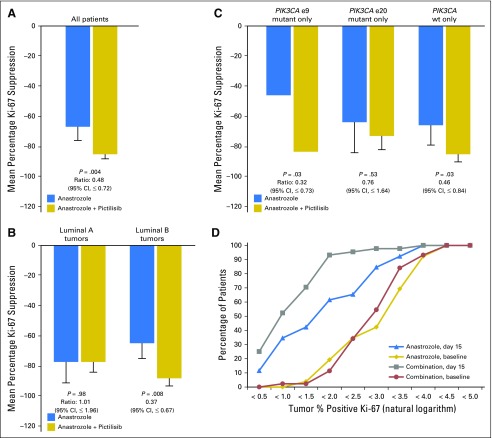
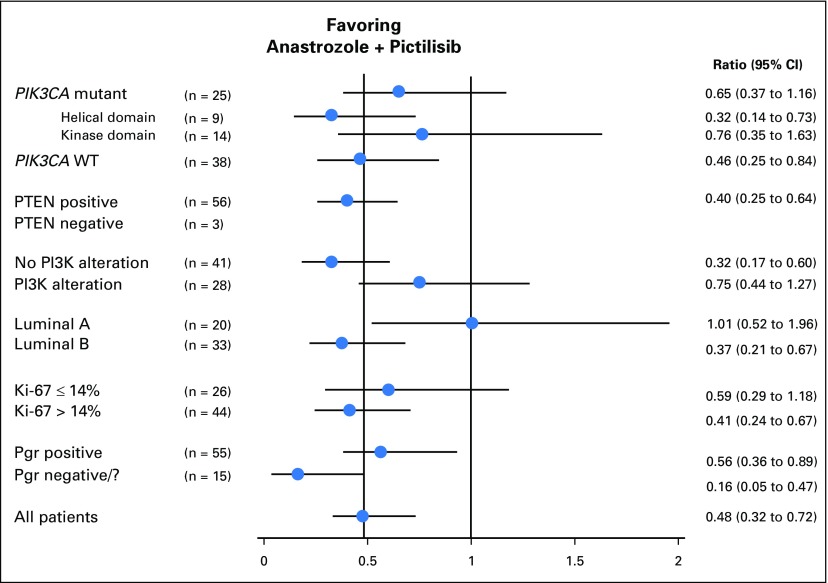
Results: There was significantly greater geometric mean Ki-67 suppression of 83.8% (one-sided 95% CI, ≥ 79.0%) for the combination and 66.0% (95% CI, ≤ 75.4%) for anastrozole (geometric mean ratio [combination:anastrozole], 0.48; 95% CI, ≤ 0.72; P = .004). PIK3CA mutations were not predictive of response to pictilisib, but there was significant interaction between response to treatment and molecular subtype (P = .03); for patients with luminal B tumors, the combination:anastrozole geometric mean ratio of Ki-67 suppression was 0.37 (95% CI, ≤ 0.67; P = .008), whereas no significant Ki-67 response was observed for pictilisib in luminal A tumors (1.01; P = .98). Multivariable analysis confirmed Ki-67 response to the combination treatment of patients with luminal B tumors irrespective of progesterone receptor status or baseline Ki-67 expression.
Conclusion: Adding pictilisib to anastrozole significantly increases suppression of tumor cell proliferation in luminal B primary breast cancer.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Window-of-Opportunity Trials in the Preoperative Setting: Insights Into Drug Development for Estrogen Receptor-Positive Breast Cancer.J Clin Oncol. 2016 Jun 10;34(17):1970-2. doi: 10.1200/JCO.2015.66.2312. Epub 2016 Mar 21. J Clin Oncol. 2016. PMID: 27001589 No abstract available.
-
Pictilisib Plus Anastrozole Reduces Proliferation in ER+ Breast Cancer.Cancer Discov. 2016 May;6(5):471. doi: 10.1158/2159-8290.CD-RW2016-055. Epub 2016 Mar 24. Cancer Discov. 2016. PMID: 27012832
-
Obviating the Need for Serial Biopsies Through Random Assignment.J Clin Oncol. 2017 Jan 10;35(2):260. doi: 10.1200/JCO.2016.69.4471. Epub 2016 Oct 31. J Clin Oncol. 2017. PMID: 28056195 No abstract available.
-
Reply to R.F. Sweis et al.J Clin Oncol. 2017 Jan 10;35(2):261-262. doi: 10.1200/JCO.2016.69.8019. Epub 2016 Oct 31. J Clin Oncol. 2017. PMID: 28056198 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
