

A patient-centered system in a provider-centered world: challenges of incorporating post-discharge wound data into practice
- PMID: 26977103
- PMCID: PMC6375197
- DOI: 10.1093/jamia/ocv183
A patient-centered system in a provider-centered world: challenges of incorporating post-discharge wound data into practice
Abstract
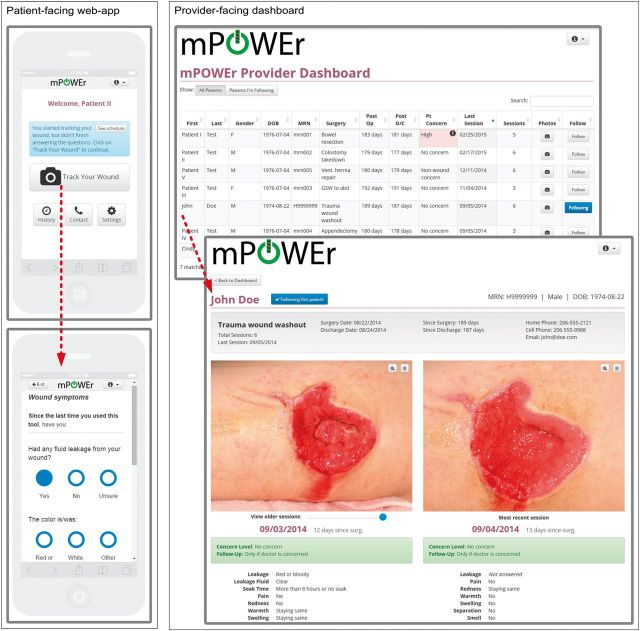
Objective: The proposed Meaningful Use Stage 3 recommendations require healthcare providers to accept patient-generated health data (PGHD) by 2017. Yet, we know little about the tensions that arise in supporting the needs of both patients and providers in this context. We sought to examine these tensions when designing a novel, patient-centered technology - mobile Post-Operative Wound Evaluator (mPOWEr) - that uses PGHD for post-discharge surgical wound monitoring.
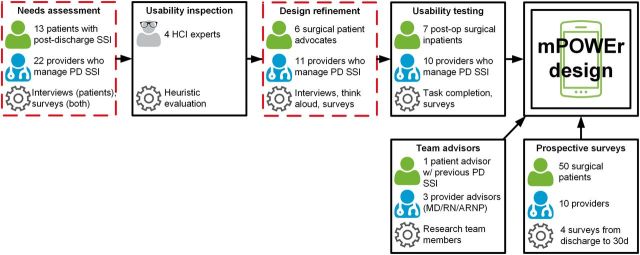
Materials and methods: As part of the iterative design process of mPOWEr, we conducted semistructured interviews and think-aloud sessions using mockups with surgical patients and providers. We asked participants how mPOWEr could enhance the current post-discharge process for surgical patients, then used grounded theory to develop themes related to conflicts and agreements between patients and providers.
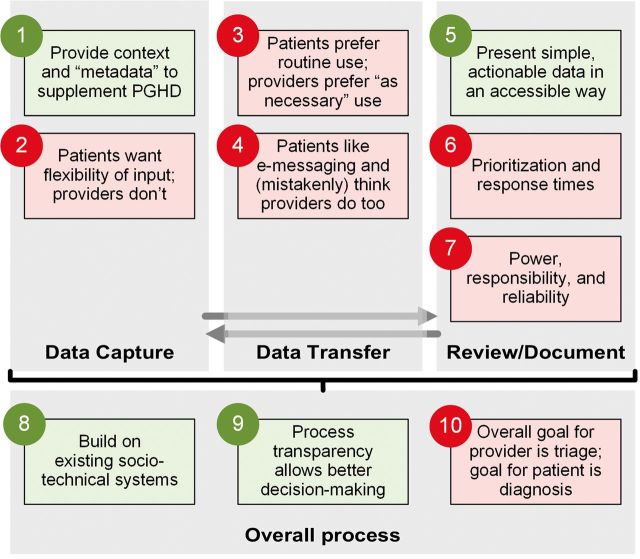
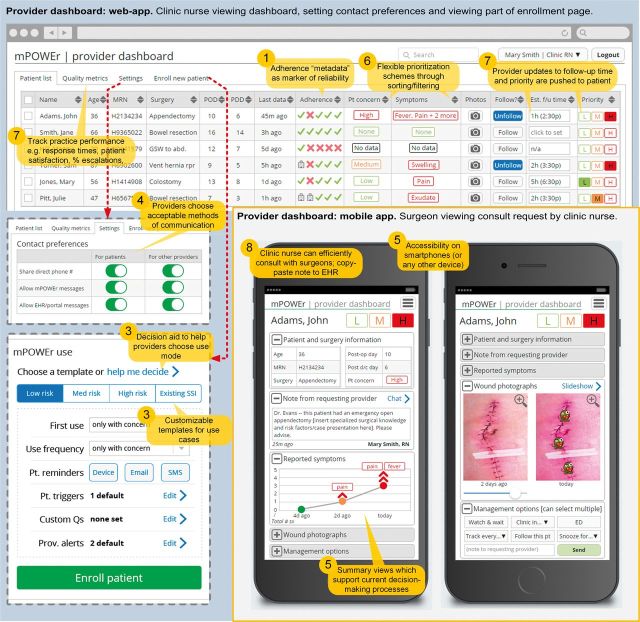
Results: We identified four areas of agreement: providing contextual metadata, accessible and actionable data presentation, building on existing sociotechnical systems, and process transparency. We identified six areas of conflict, with patients preferring: more flexibility in data input, frequent data transfer, text-based communication, patient input in provider response prioritization, timely and reliable provider responses, and definitive diagnoses.
Discussion: We present design implications and potential solutions to the identified conflicts for each theme, illustrated using our work on mPOWEr. Our experience highlights the importance of bringing a variety of stakeholders, including patients, into the design process for PGHD applications.
Conclusion: We have identified critical barriers to integrating PGHD into clinical care and describe design implications to help address these barriers. Our work informs future efforts to ensure the smooth integration of essential PGHD into clinical practice.
Keywords: dissent and disputes; mobile health; patient engagement; patient-centered care; surgical wound infection.
© The Author 2016. Published by Oxford University Press on behalf of the American Medical Informatics Association. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures

References
-
- Appelboom G, LoPresti M, Reginster J-Y, et al. The quantified patient: a patient participatory culture. Curr Med Res Opin. 2014;30:2585–2587. - PubMed
-
- Kendall L, Morris D, DT Blood Pressure Beyond the Clinic: Rethinking a Health Metric for Everyone. In: Proceedings of ACM CHI 2015. 2015: In press.
-
- DHHS. Electronic Health Record (EHR) Incentive Programs – Stage 3. 2014. http://www.reginfo.gov/public/do/eAgendaViewRule?pubId=201410&RIN=0938-AS26. Accessed January 20, 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
