

Self-reported Mobility in Older Patients Predicts Early Postoperative Outcomes after Elective Noncardiac Surgery
- PMID: 26978144
- PMCID: PMC5201172
- DOI: 10.1097/ALN.0000000000001011
Self-reported Mobility in Older Patients Predicts Early Postoperative Outcomes after Elective Noncardiac Surgery
Abstract
Background: Specific geriatric assessment tools may complement traditional perioperative risk stratification. The aim of this study was to evaluate whether self-reported mobility is predictive of postoperative outcomes in older patients undergoing elective noncardiac surgery.
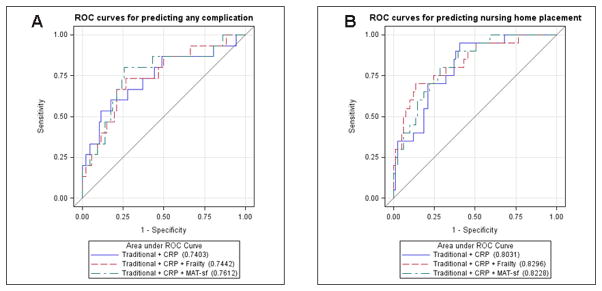
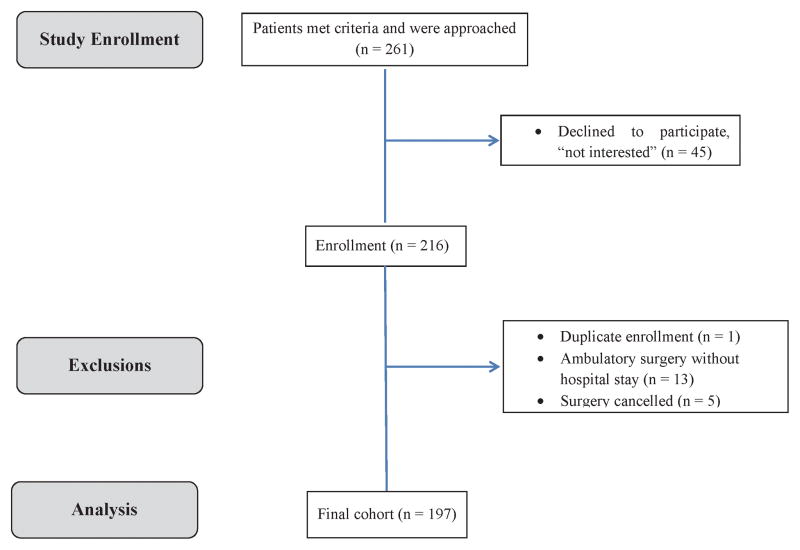
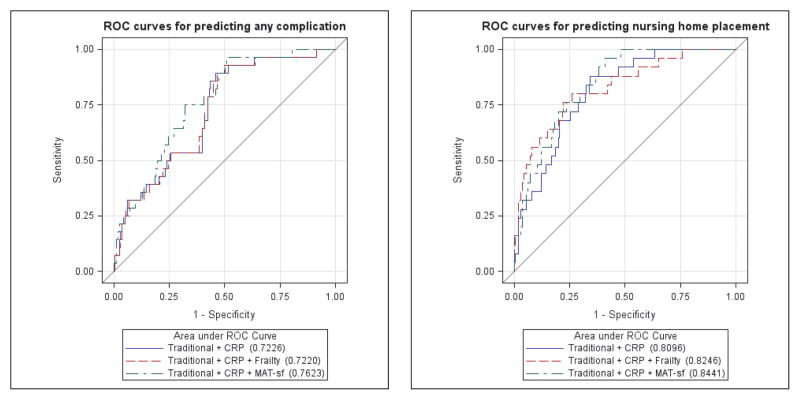
Methods: Patients aged 69 yr or older (n = 197) underwent (1) traditional risk assessments (American Society of Anesthesiologists physical status classification and Revised Cardiac Risk Index), (2) five-point frailty evaluation, (3) self-reported mobility assessment using the Mobility Assessment Tool-short form (range, 30.21 [poor] to 69.76 [excellent]), and (4) measurements of high-sensitivity C-reactive protein. Outcomes were postoperative complications, time to discharge, and nursing home placement (NHP).
Results: In the sample of this study (mean age, 75 ± 5 yr; 51% women), 72% had intermediate- or high-risk surgery. Median time to discharge was 3 days (interquartile range, 1 to 4 days). Thirty patients (15%) developed postoperative complications, and 27 (13%) required NHP. After controlling for age, sex, body mass index, pain score, Revised Cardiac Risk Index, American Society of Anesthesiologist physical status, surgical risk, and high-sensitivity C-reactive protein, worse self-reported mobility (per 10-point decrease in Mobility Assessment Tool, which is equivalent to 1 SD) was associated with more postoperative complications (odds ratio [OR], 1.69; 95% CI, 1.05 to 2.73), later time to discharge (hazards ratio, 0.81; 95% CI, 0.68 to 0.96), and increased NHP (OR, 2.01; 95% CI, 1.13 to 3.56). By using the same model, intermediate frailty or frailty increased NHP (OR, 3.11; 95% CI, 1.02 to 9.54) but was not related to either postoperative complications or time to discharge.
Conclusions: Preoperative self-reported mobility using a novel and brief assessment may help identify elderly patients at risk for adverse postoperative events.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Etzioni DA, Liu JH, O’Connell JB, Maggard MA, Ko CY. Elderly patients in surgical workloads: a population-based analysis. Am Surg. 2003;69:961–5. - PubMed
-
- Buldu I, Tepeler A, Karatag T, Bodakci MN, Hatipoglu NK, Penbegul N, Akman T, Istanbulluoglu O, Armagan A. Does aging affect the outcome of percutaneous nephrolithotomy? Urolithiasis. 2015;43:183–7. - PubMed
-
- Chung F, Mezei G. Adverse outcomes in ambulatory anesthesia. Can J Anaesth. 1999;46:R18–34. - PubMed
-
- Tiret L, Hatton F, Desmonts JM, Vourc'h G. Prediction of outcome of anaesthesia in patients over 40 years: a multifactorial risk index. Stat Med. 1988;7:947–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
