

Post-discharge Follow-up Characteristics Associated With 30-Day Readmission After Heart Failure Hospitalization
- PMID: 26978568
- PMCID: PMC4800825
- DOI: 10.1097/MLR.0000000000000492
Post-discharge Follow-up Characteristics Associated With 30-Day Readmission After Heart Failure Hospitalization
Abstract
Background: Readmission within 30 days after hospitalization for heart failure (HF) is a major public health problem.
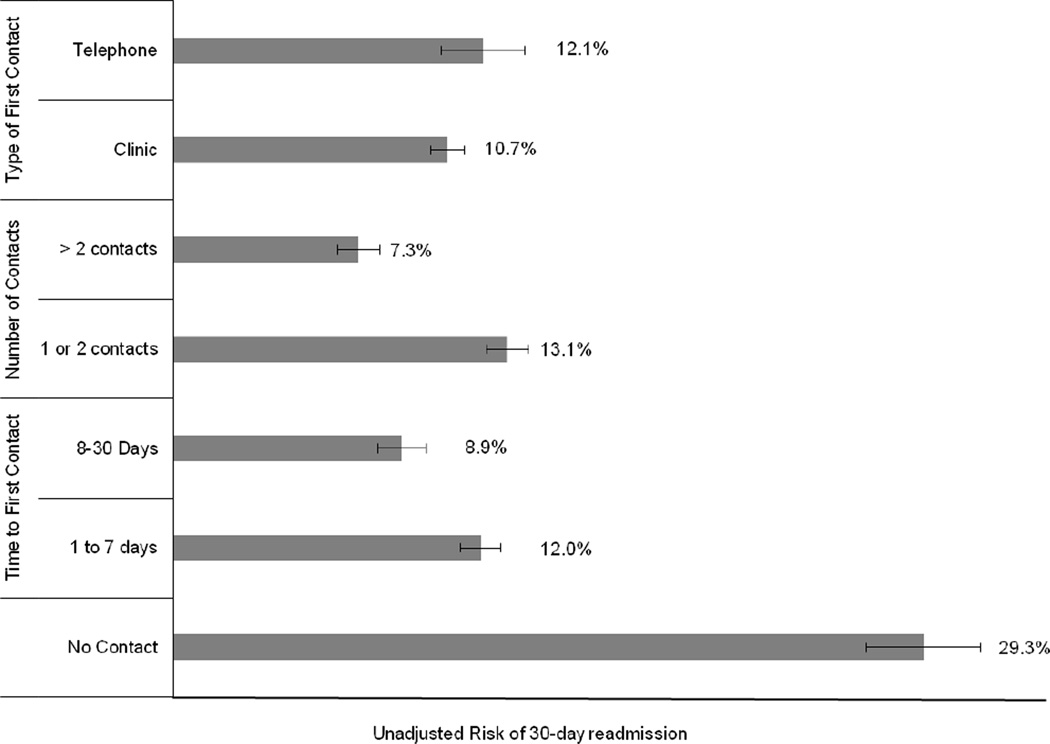
Objective: To examine whether timing and type of post-discharge follow-up impacts risk of 30-day readmission in adults hospitalized for HF.
Design: Nested matched case-control study (January 1, 2006-June 30, 2013).
Setting: A large, integrated health care delivery system in Northern California.
Participants: Hospitalized adults with a primary diagnosis of HF discharged to home without hospice care.
Measurements: Outpatient visits and telephone calls with cardiology and general medicine providers in non-emergency department and non-urgent care settings were counted as follow-up care. Statistical adjustments were made for differences in patient sociodemographic and clinical characteristics, acute severity of illness, hospitalization characteristics, and post-discharge medication changes and laboratory testing.
Results: Among 11,985 eligible adults, early initial outpatient contact within 7 days after discharge was associated with lower odds of readmission [adjusted odds ratio (OR)=0.81; 95% CI, 0.70-0.94], whereas later outpatient contact between 8 and 30 days after hospital discharge was not significantly associated with readmission (adjusted OR=0.99; 95% CI, 0.82-1.19). Initial contact by telephone was associated with lower adjusted odds of 30-day readmission (adjusted OR=0.85; 95% CI, 0.69-1.06) but was not statistically significant.
Conclusions: In adults discharged to home after hospitalization for HF, outpatient follow-up with a cardiology or general medicine provider within 7 days was associated with a lower chance of 30-day readmission.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB American Heart Association Statistics C, Stroke Statistics S. Heart disease and stroke statistics--2012 update: A report from the american heart association. Circulation. 2012;125:e2–e220. - PMC - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Pina IL, Trogdon JG on behalf of the American Heart Association Advocacy Coordinating Committee CoAT, Vascular Biology CoCR, Intervention CoCCCoE, Pr. Forecasting the impact of heart failure in the united states: A policy statement from the american heart association. Circulation. Heart failure. 2013 - PMC - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the medicare fee-for-service program. The New England journal of medicine. 2009;360:1418–1428. - PubMed
-
- Keenan PS, Normand SL, Lin Z, Drye EE, Bhat KR, Ross JS, Schuur JD, Stauffer BD, Bernheim SM, Epstein AJ, Wang Y, Herrin J, Chen J, Federer JJ, Mattera JA, Wang Y, Krumholz HM. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circulation. Cardiovascular quality and outcomes. 2008;1:29–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
