

Evidence of surgical outcomes fluctuates over time: results from a cumulative meta-analysis of laparoscopic versus open appendectomy for acute appendicitis
- PMID: 26979491
- PMCID: PMC4793521
- DOI: 10.1186/s12876-016-0453-0
Evidence of surgical outcomes fluctuates over time: results from a cumulative meta-analysis of laparoscopic versus open appendectomy for acute appendicitis
Abstract
Background: In surgical trials, complex variables such as equipment development and surgeons' learning curve are involved. The evidence obtained in these trials can thus fluctuate over time. We explored the stability of the evidence obtained during surgery by conducting a cumulative meta-analysis of randomized controlled trials for open and laparoscopic appendectomy.
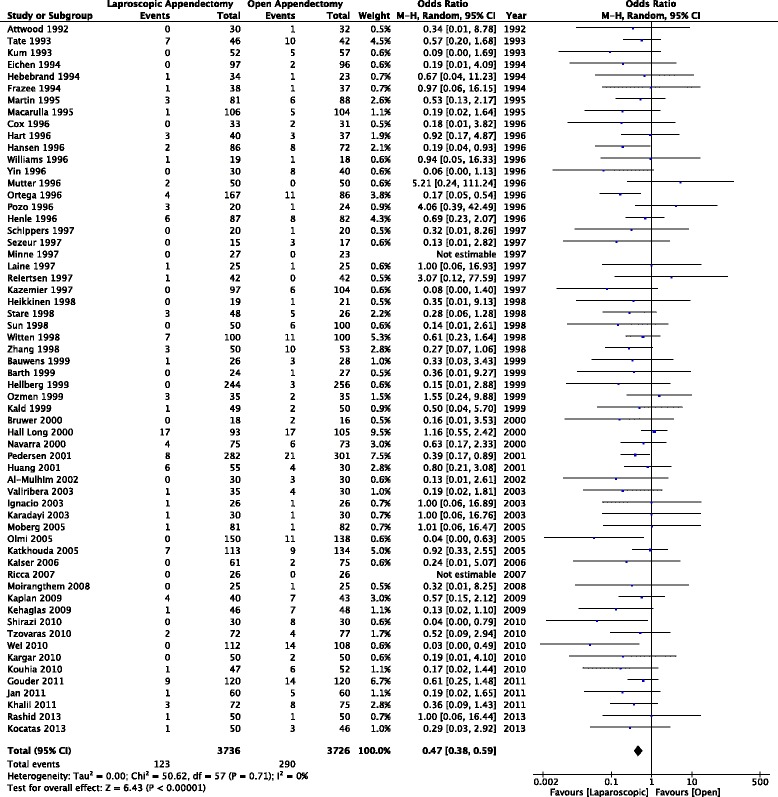
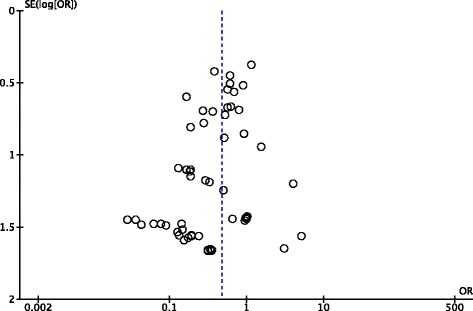
Methods: We conducted a cumulative meta-analysis of randomized controlled trials comparing laparoscopic appendectomy with open appendectomy for acute appendicitis, a topic with the greatest number of trials in the gastroenterological surgical field. We searched the MEDLINE (PubMed), EMBASE, and CINAHL databases up to September 2014 and reviewed the bibliographies. Outcomes were the incidence of intra-abdominal abscess, incidence of wound infection, operative time, and length of hospital stay. We used the 95 % confidence interval (95 % CI) of effect size for the significance test.
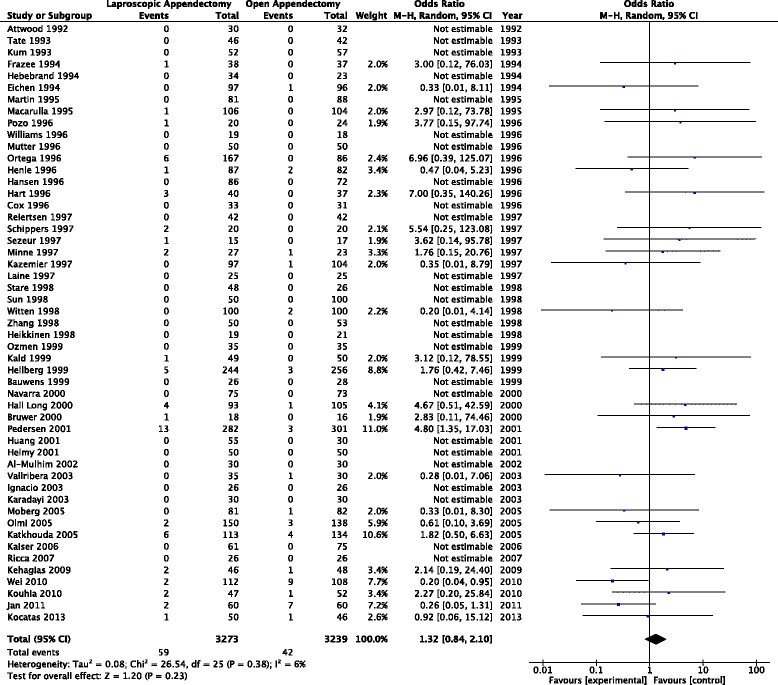
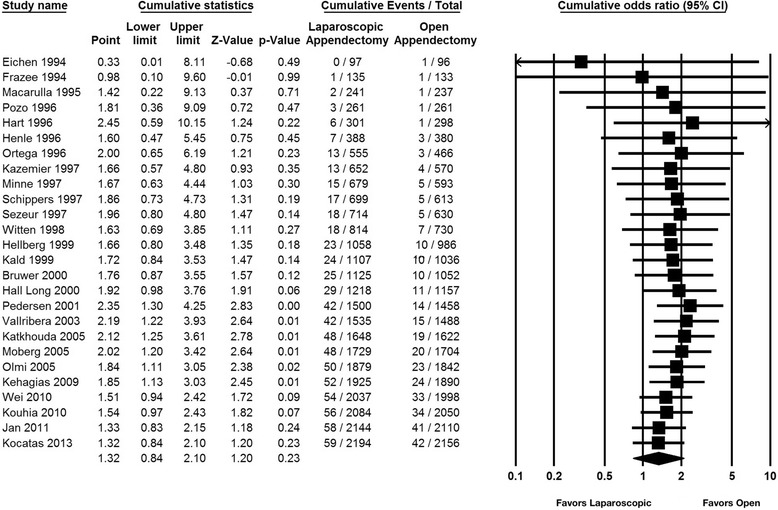
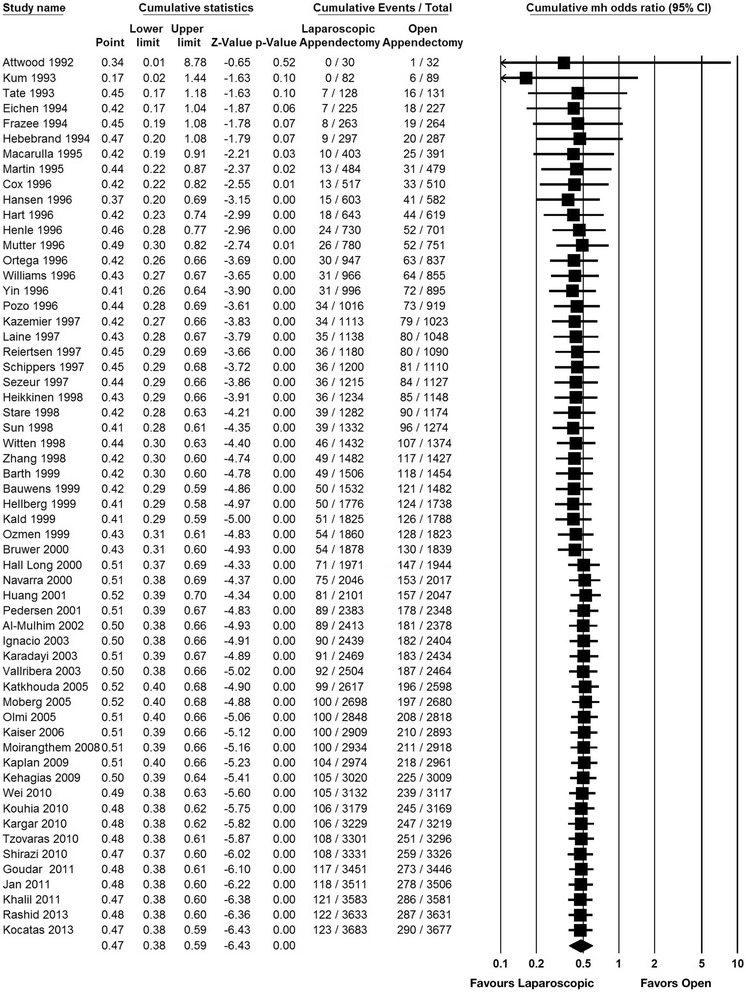
Results: Sixty-four trials were included in this analysis. Of the 51 trials addressing intra-abdominal abscesses, our cumulative meta-analysis of trials published up to and including 2001 demonstrated statistical significance in favor of open appendectomy (cumulative odds ratio [OR] 2.35, 95 % CI 1.30-4.25). The effect size in favor of open procedures began to disappear after 2001, leading to an insignificant result with an overall cumulative OR of 1.32 (95 % CI 0.84-2.10) when laparoscopic appendectomy was compared with open appendectomy.
Conclusions: The evidence regarding treatment effectiveness changed over time, after treatment effectiveness became significant in trials comparing laparoscopic and open appendectomy. Observing only the 95 % confidence interval of effect size from a meta-analysis may not provide conclusive results.
Keywords: Cumulative meta-analysis; Laparoscopic appendectomy; Open appendectomy; Randomized controlled trials.
Figures

References
-
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2700. - PMC - PubMed
-
- Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico (GISSI). Lancet. 1986;1:397–402. - PubMed
-
- Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet. 1988;2:349–360. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
