

Tuberculosis as a three-act play: A new paradigm for the pathogenesis of pulmonary tuberculosis
- PMID: 26980490
- PMCID: PMC4795183
- DOI: 10.1016/j.tube.2015.11.010
Tuberculosis as a three-act play: A new paradigm for the pathogenesis of pulmonary tuberculosis
Abstract
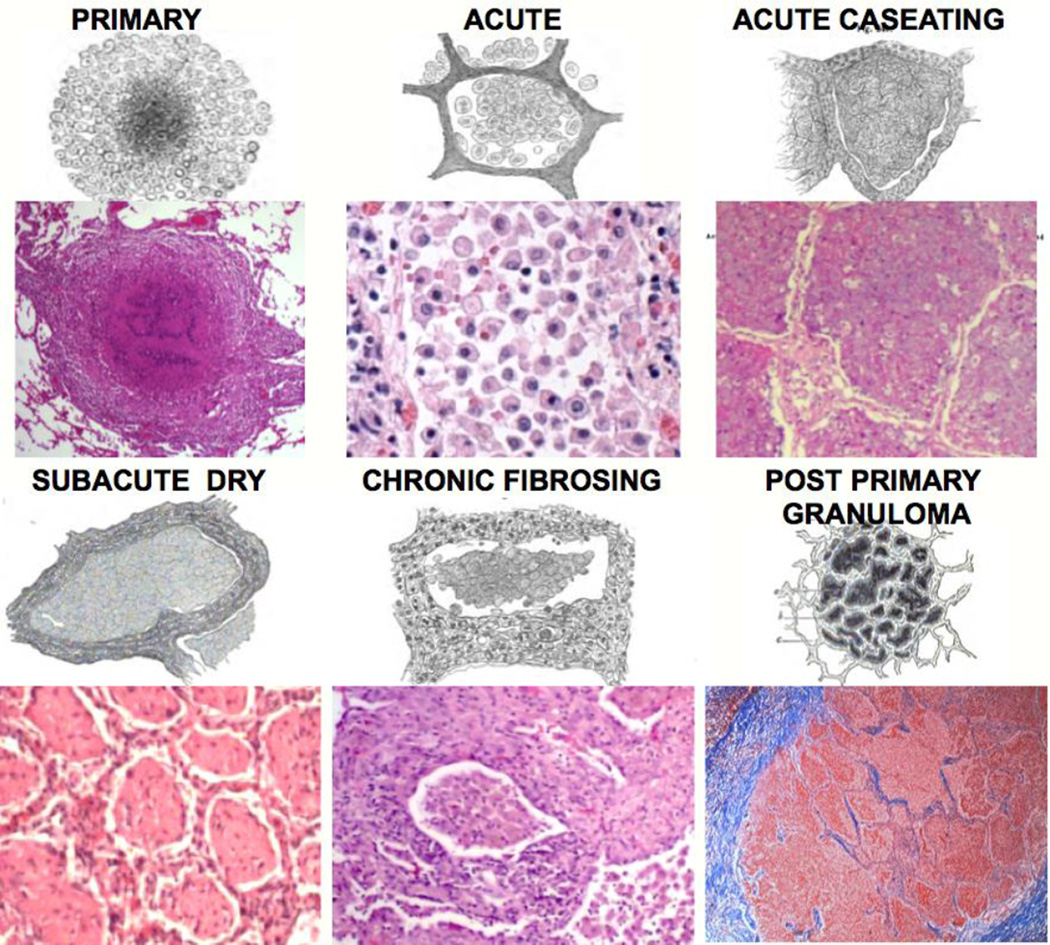
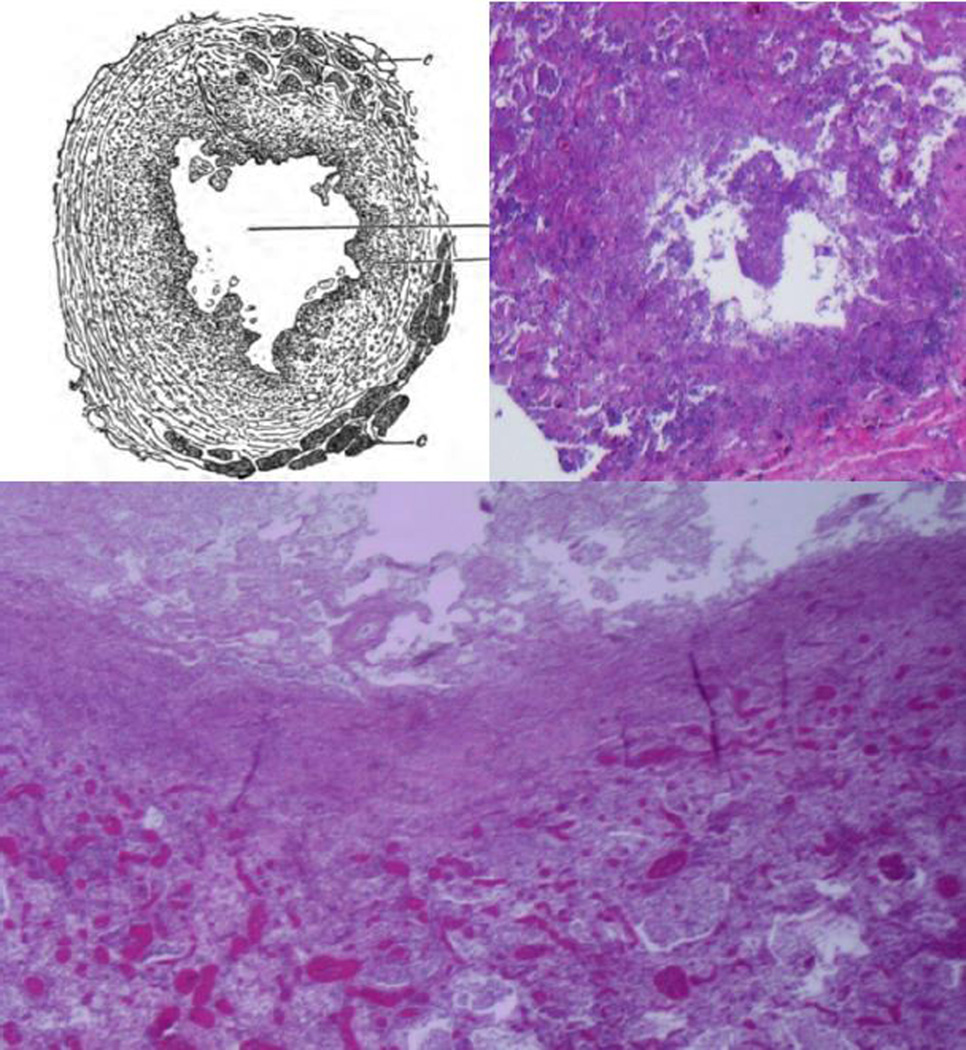
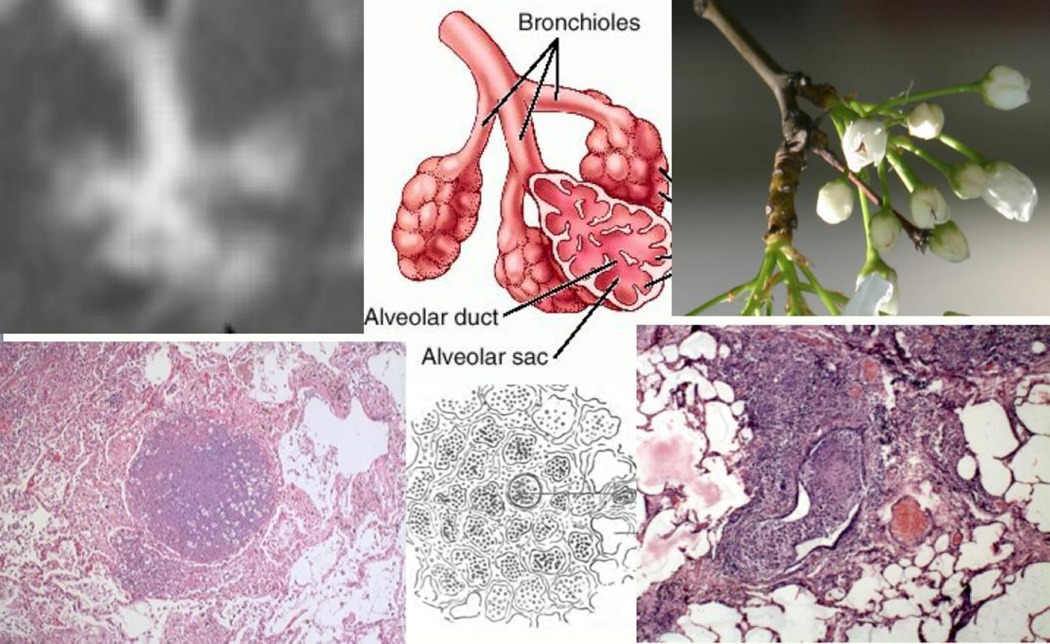
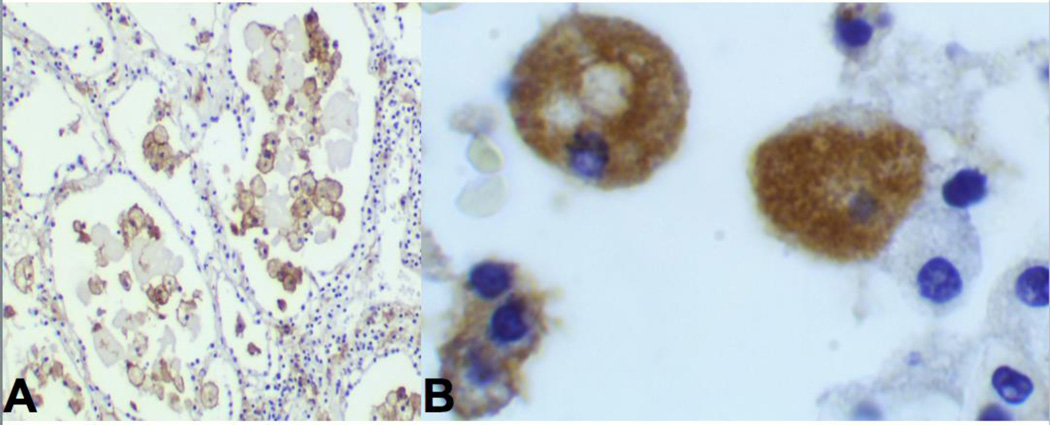
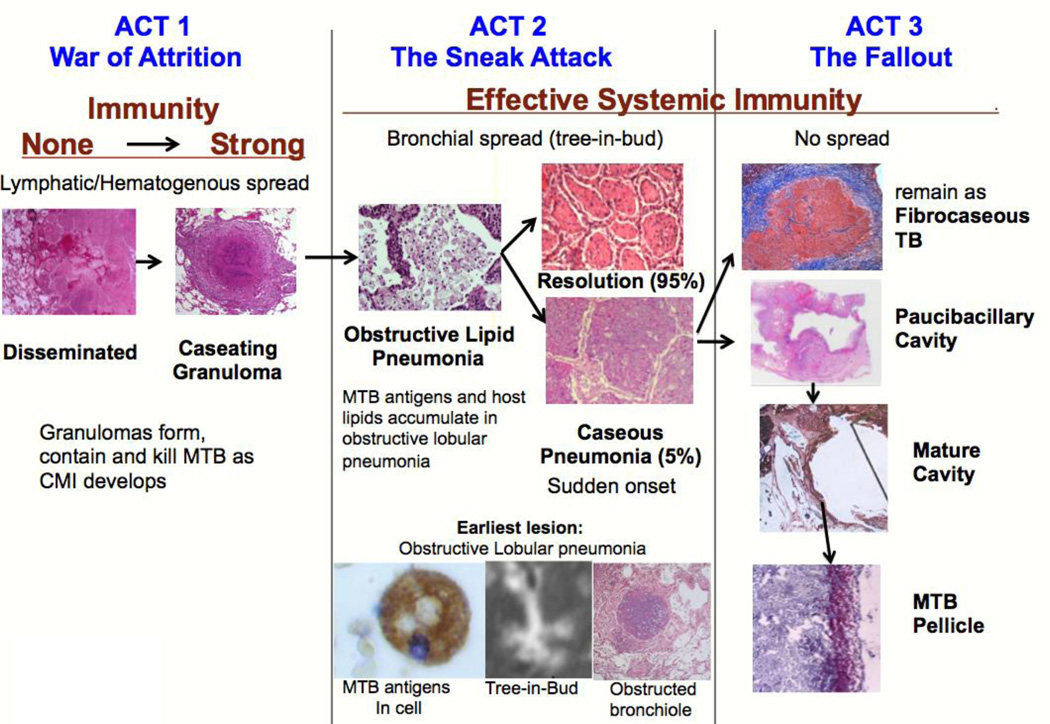
Lack of access to human tissues with untreated tuberculosis (TB) has forced generations of researchers to use animal models and to adopt a paradigm that granulomas are the characteristic lesion of both primary and post primary TB. An extended search of studies of human lung tissues failed to find any reports that support this paradigm. We found scores of publications from gross pathology in 1804 through high resolution CT scans in 2015 that identify obstructive lobular pneumonia, not granulomas, as the characteristic lesion of developing post-primary TB. This paper reviews this literature together with other relevant observations to formulate a new paradigm of TB with three distinct stages: a three-act play. First, primary TB, a war of attrition, begins with infection that spreads via lymphatics and blood stream before inducing systemic immunity that contains and controls the organisms within granulomas. Second, post-primary TB, a sneak attack, develops during latent TB as an asymptomatic obstructive lobular pneumonia in persons with effective systemic immunity. It is a paucibacillary process with no granulomas that spreads via bronchi and accumulates mycobacterial antigens and host lipids for 1-2 years before suddenly undergoing caseous necrosis. Third, the fallout, is responsible for nearly all clinical post primary disease. It begins with caseous necrotic pneumonia that is either retained to become the focus of fibrocaseous disease or is coughed out to leave a cavity. This three-stage paradigm suggests testable hypotheses and plausible answers to long standing questions of immunity to TB.
Keywords: Cavity; Human; Lung; Pathogenesis; Pathology; Post primary.
Copyright © 2015 The Author. Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Kaufmann SH, Evans TG, Hanekom WA. Tuberculosis vaccines: time for a global strategy. Sci Transl Med. 2015;7:276fs8. - PubMed
-
- Hunter RL, Jagannath C, Actor JK. Pathology of postprimary tuberculosis in humans and mice: contradiction of long-held beliefs. Tuberculosis (Edinb) 2007;87:267–278. - PubMed
-
- Hunter RL, Actor JK, Hwang S, Karev V, Jagannath C. Pathogenesis of Post Primary Tuberculosis: Immunity and Hypersensitivity in the Development of Cavities. Ann Clin Lab Sci. 2014;44:365–387. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
