

Systemic inflammation in a melanoma patient treated with immune checkpoint inhibitors-an autopsy study
- PMID: 26981243
- PMCID: PMC4791920
- DOI: 10.1186/s40425-016-0117-1
Systemic inflammation in a melanoma patient treated with immune checkpoint inhibitors-an autopsy study
Abstract
Background: Immune checkpoint inhibitors targeting cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1) have been recently approved for treatment of patients with metastatic melanoma and non-small cell lung cancer (NSCLC). Despite important clinical benefits, these therapies are associated with a diverse spectrum of immune-related adverse events (irAEs) that are typically transient, but occasionally severe or even fatal.
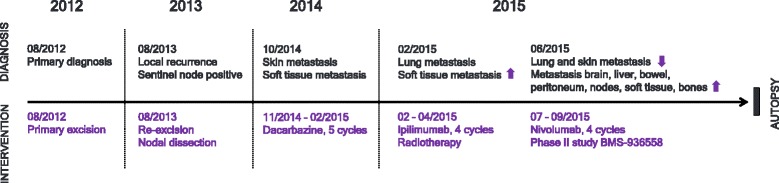
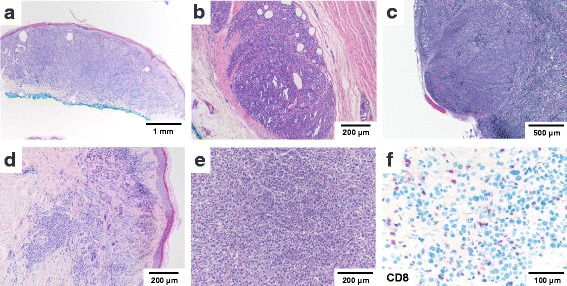
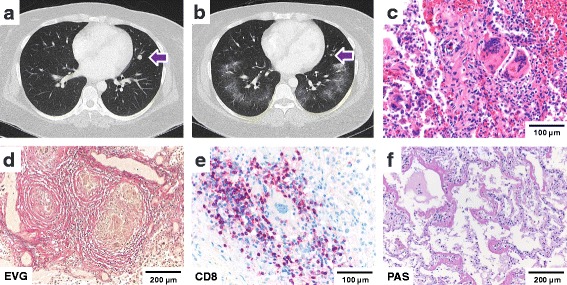
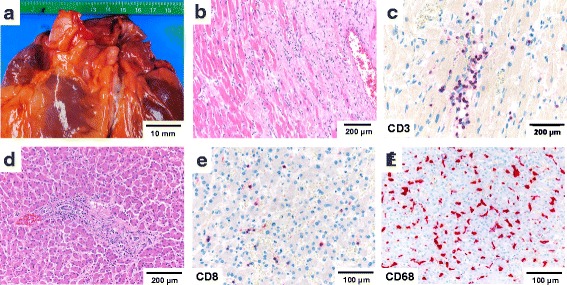
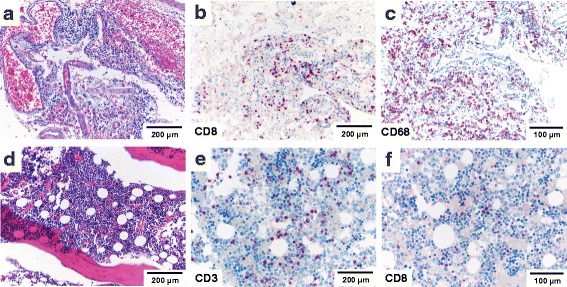
Case presentation: This autopsy case illustrates that clinically overt irAEs may represent only a fraction of the total spectrum of immune-related organ pathology in patients treated with immune checkpoint inhibitors. We report a comprehensive analysis of systemic irAE pathology based on the autopsy of a 35-year-old female patient with metastatic melanoma treated first with ipilimumab and then nivolumab. The clinical course was characterized by a mixed tumor response with regression of skin and lung metastases and fatal progression of metastatic disease in the small bowel, peritoneum and brain. During therapy with ipilimumab, radiographic features of immune-related pneumonitis were noted. The autopsy examination established a sarcoid-like granulomatous reaction of the lung, pulmonary fibrosis and diffuse alveolar damage. Importantly, a clinically unapparent but histologically striking systemic inflammation involving the heart, central nervous system, liver and bone marrow was identified. Severe immune-related end-organ damage due to lymphocytic myocarditis was found.
Conclusions: Autopsy studies are an important measure of quality control and may identify clinically unapparent irAEs in patients treated with immunotherapy. Pathologists and clinicians need to be aware of the broad spectrum of irAEs for timely management of treatment-related morbidity.
Keywords: Anti-tumor T cell response; Antibody; Autoimmunity; Autopsy; Immune checkpoint inhibitors; Immunotherapy; Ipilimumab; Melanoma; Nivolumab.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials