

Uniportal video-assisted thoracoscopic bronchoplastic and carinal sleeve procedures
- PMID: 26981273
- PMCID: PMC4775265
- DOI: 10.3978/j.issn.2072-1439.2016.01.76
Uniportal video-assisted thoracoscopic bronchoplastic and carinal sleeve procedures
Abstract
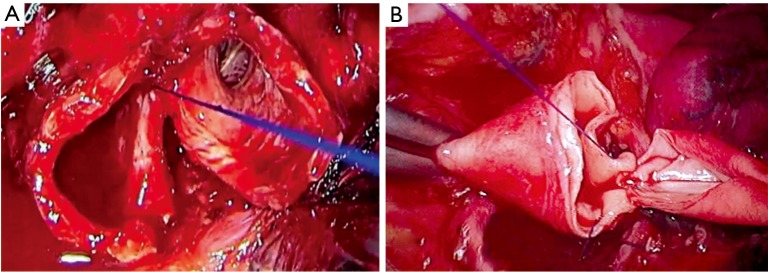
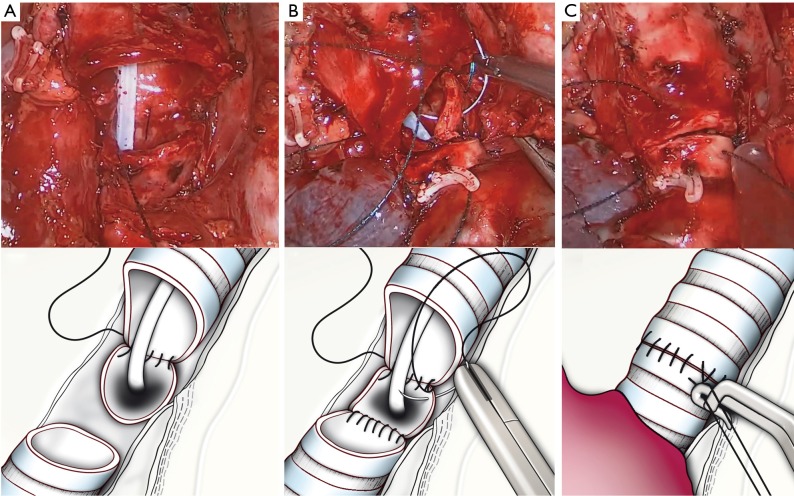
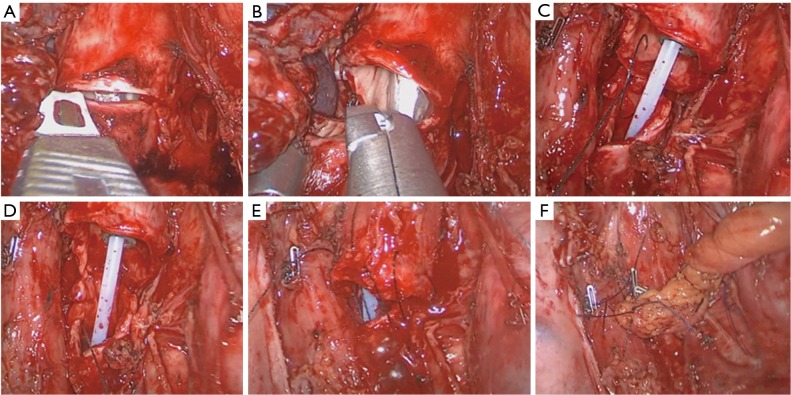
Despite of the recent advanced with the video-assisted thoracoscopic surgery (VATS), the most common approach for bronchial and carinal resection is still the open surgery. The technical difficulties, the steep learning curve and the concerns about performing an oncologic and safe reconstruction in advanced cases, are the main reasons for the low adoption of VATS for sleeve resections. Most of the authors use 3-4 incisions for thoracoscopic sleeve procedures. However these surgical techniques can be performed by a single incision approach by skilled uniportal VATS surgeons. The improvements of the surgical instruments, high definition cameras and recent 3D systems have greatly contributed to facilitate the adoption of uniportal VATS techniques for sleeve procedures. In this article we describe the technique of thoracoscopic bronchial sleeve, bronchovascular and carinal resections through a single incision approach.
Keywords: Sleeve lobectomy; bronchoplasty; carinal resection; double sleeve; uniportal video-assisted thoracoscopic surgery (VATS); vascular reconstruction.
Conflict of interest statement
Figures






References
-
- Villamizar NR, Darrabie MD, Burfeind WR, et al. Thoracoscopic lobectomy is associated with lower morbidity compared with thoracotomy. J Thorac Cardiovasc Surg 2009;138:419-25. - PubMed
-
- Swanson SJ, Herndon JE, 2nd, D'Amico TA, et al. Video-assisted thoracic surgery lobectomy: report of CALGB 39802da prospective, multi-institution feasibility study. J Clin Oncol 2007;25:4993-7. - PubMed
-
- McKenna RJ, Jr, Houck W, Fuller CB. Video-assisted thoracic surgery lobectomy: experience with 1,100 cases. Ann Thorac Surg 2006;81:421-5; discussion 425-6. - PubMed
-
- Kaseda S, Aoki T, Hangai N, et al. Better pulmonary function and prognosis with video-assisted thoracic surgery than with thoracotomy. Ann Thorac Surg 2000;70:1644-6. - PubMed
-
- Yang X, Wang S, Qu J. Video-assisted thoracic surgery (VATS) compares favorably with thoracotomy for the treatment of lung cancer: a five-year outcome comparison. World J Surg 2009;33:1857-61. - PubMed
LinkOut - more resources
Full Text Sources