

Objective Evaluation of Vergence Disorders and a Research-Based Novel Method for Vergence Rehabilitation
- PMID: 26981330
- PMCID: PMC4790421
- DOI: 10.1167/tvst.5.2.8
Objective Evaluation of Vergence Disorders and a Research-Based Novel Method for Vergence Rehabilitation
Abstract
Purpose: We performed video-oculography to evaluate vergence eye movement abnormalities in students diagnosed clinically with vergence disorders. We tested the efficiency of a novel rehabilitation method and evaluated its benefits with video-oculography cross-correlated with clinical tests and symptomatology.
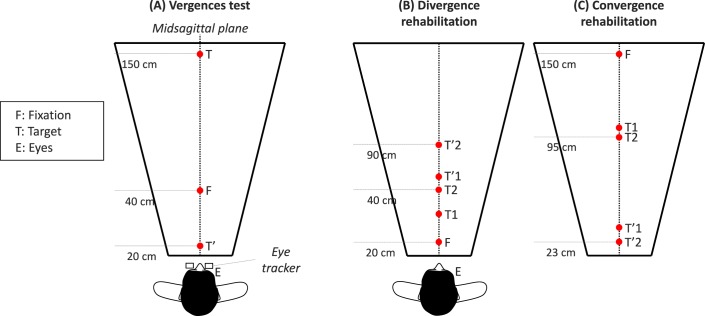
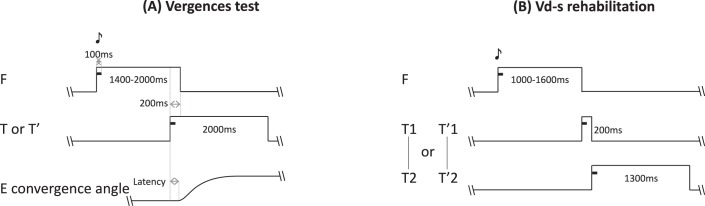
Methods: A total of 19 students (20-27 years old) underwent ophthalmologic, orthoptic examination, and a vergence test coupled with video-oculography. Eight patients were diagnosed with vergence disorders with a high symptomatology score (CISS) and performed a 5-week session of vergence rehabilitation. Vergence and rehabilitation tasks were performed with a trapezoid surface of light emitting diodes (LEDs) and adjacent buzzers (US 8851669). We used a novel Vergence double-step (Vd-s) protocol: the target stepped to a second position before the vergence movement completion. Afterward the vergence test was repeated 1 week and 1 month later.
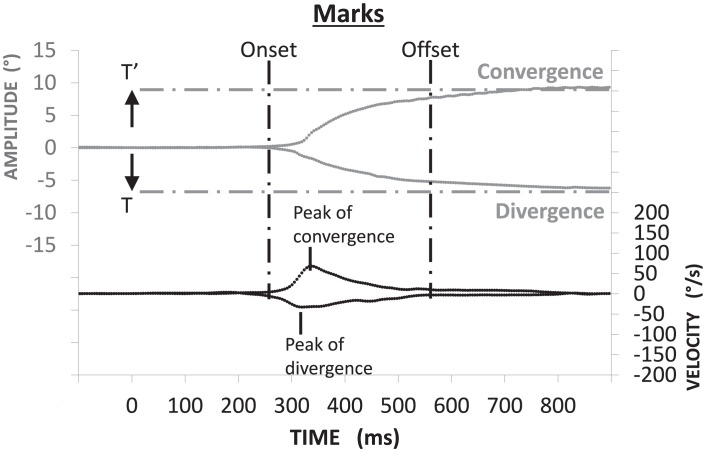
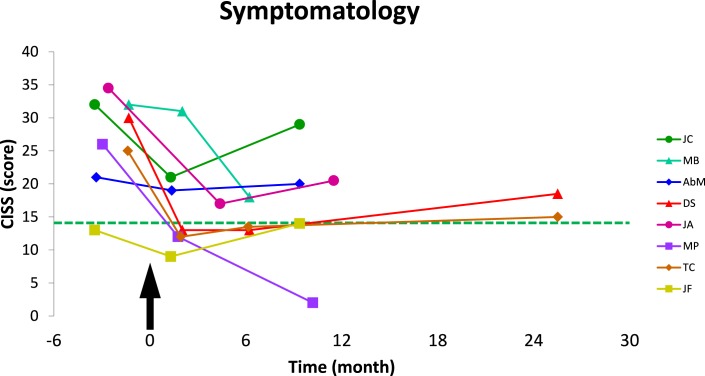
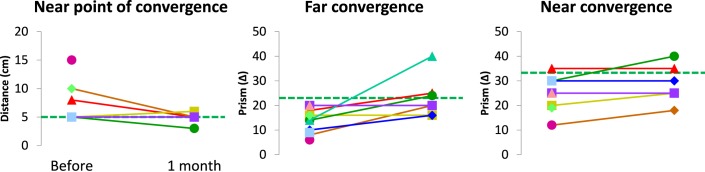
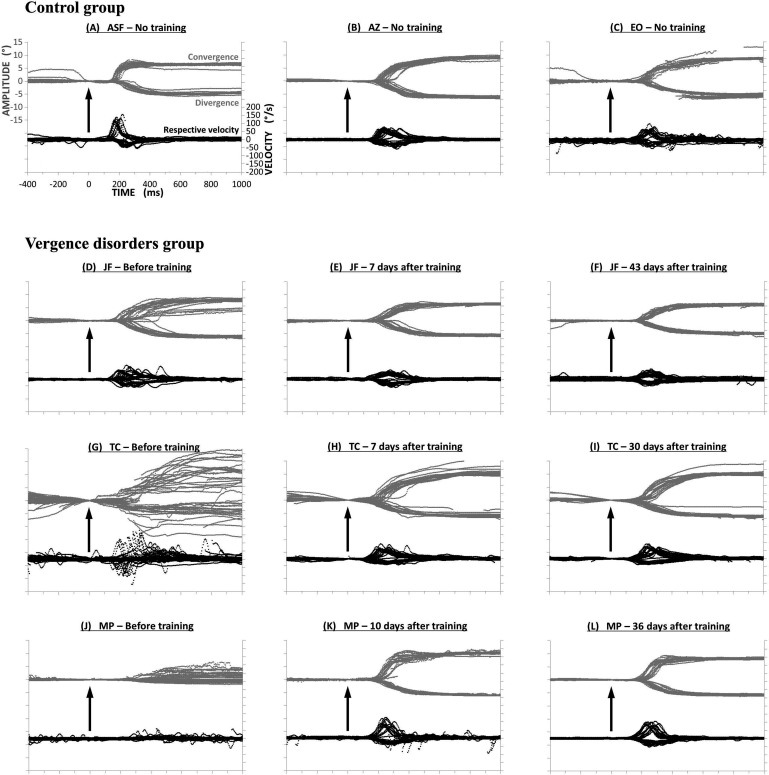
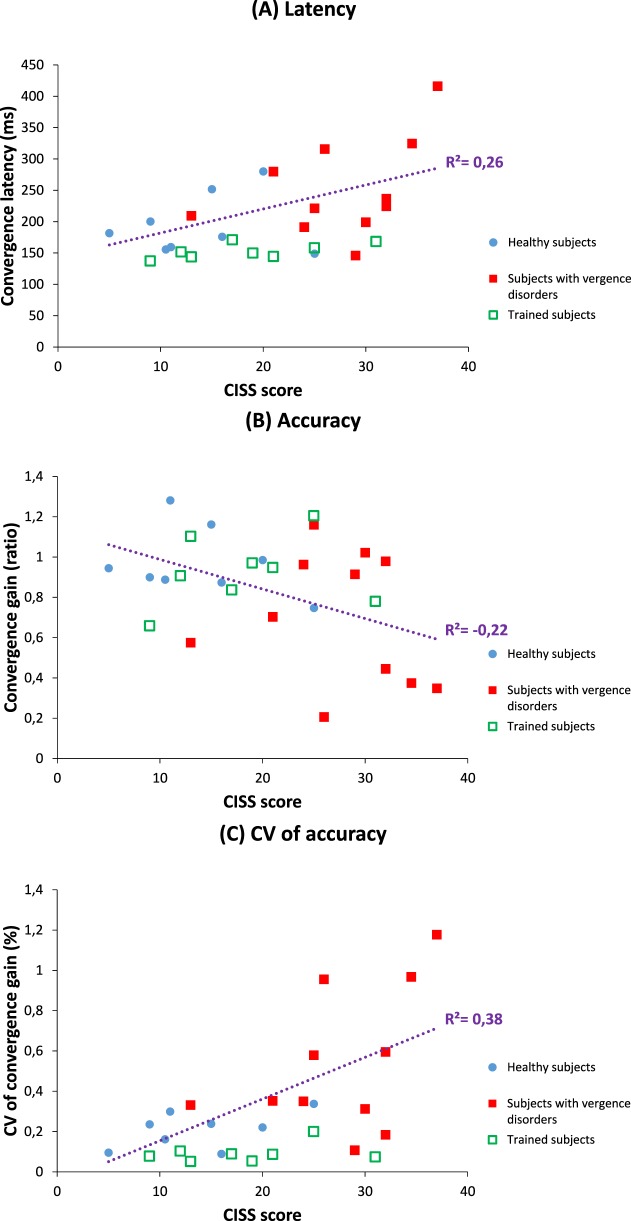
Results: Abnormally increased intertrial variability was observed for many vergence parameters (gain, duration, and speed) for the subjects with vergence disorders. High CISS scores were correlated with variability and increased latency. After the Vd-s, variability of all parameters dropped to normal or better levels. Moreover, the convergence and divergence latency diminished significantly to levels better than normal; benefits were maintained 1 month after completion of Vd-s. CISS scores dropped to normal level, which was maintained up to 1 year.
Conclusions and translational relevance: Intertrial variability is the major marker of vergence disorders. The Vd-s research-based method leads to normalization of vergence properties and lasting removal of symptoms. The efficiency of the method is due to the spatiotemporal parameters of repetitive trials that stimulate neural plasticity.
Keywords: accommodation; binocular vision/stereopsis; double-step task; rehabilitation; vergence.
Figures
References
-
- Montés-Micó R. Prevalence of general dysfunctions in binocular vision. Ann Ophthalmol. 2001; 33: 205–208.
-
- Lavrich JB. Convergence insufficiency and its current treatment. Curr Opin Ophthalmol. 2010; 21: 356–360. - PubMed
-
- Scheiman M,, Cooper J,, Mitchell GL,, et al. A survey of treatment modalities for convergence insufficiency. Optom Vis Sci. 2002; 79: 151–157. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
